Slate Reports on Different Types of LDLs
As a follow-up to my post "The Truth About Cholesterol", here's a report from Slate showing that all LDLs are not created equal, and some types are more dangerous than others. Moreover, the article discusses how America's "War on Fat" steered us away from butter and lard, but led us to an arguably more dangerous food, the refined carbohydrate. Post your thoughts!
As a follow-up to my post "The Truth About Cholesterol", here's a report from Slate showing that all LDLs are not created equal, and some types are more dangerous than others. Moreover, the article discusses how America's "War on Fat" steered us away from butter and lard, but led us to an arguably more dangerous food, the refined carbohydrate. Post your thoughts!
The Truth About Cholesterol
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
Second, the LDL value doesn't tell the whole story. After all, some people that have low LDL levels, still develop heart disease. When your doctor orders a standard lipid panel, LDLs are measured along with other lipids, such as high-density lipoprotein (HDL) cholesterol and triglycerides. What role do these other types of lipids play in cardiovascular health?
Let's start with the first question: Do higher doses of the drug really improve outcomes? This idea popped into my mind while reading a recent study in PLoS One that looked at LDL levels in patients diagnosed with familial hypercholesterolemia, a genetic predisposition to high levels of “bad” cholesterol. Caused by specific DNA mutations on a small region of chromosome 19, familial hypercholesterolemia drastically increases the chances that a person will develop heart disease. In fact, studies estimate that 85% of men with this mutation will have a heart attack by the age of 60.
The PLoS study found that only a minority of people with hypercholesterolemia brought their LDL levels down to recommended values, even when using statins. According to the authors, doctors were being too cautious with Lipitor dosing, and felt that higher doses would help patients reach their LDL targets.
Blood....beginning....to....boil.....
I know this isn't the first time I've climbed up on my soapbox saying “more medication is not always the answer”, but I wanted to find proof. Lo and behold, I came across a good study from the New England Journal of Medicine that calculated the risk of a major cardiovascular event depending on whether people were taking low- or high-doses of Lipitor (10 or 80 mg, respectively).
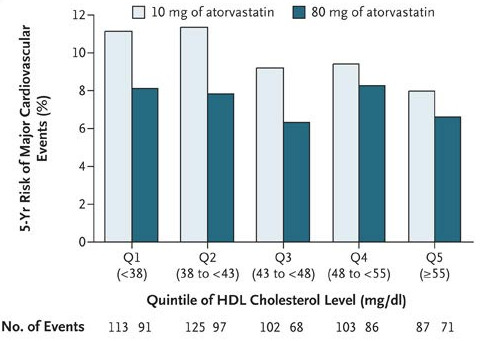
Take a look at Figure 1: Higher doses of Lipitor only made a big difference in risk when HDL levels were low. As HDL levels rose, the difference in height between the light- and dark-green bars went down. This means that if a person can get his or her “good” cholesterol high enough, higher doses of Lipitor will NOT necessarily decrease the risk of having a cardiovascular event.
This finding ties in well with the second question: What role do these other numbers play in cardiovascular health? From the NEJM study, we've seen that high HDL levels – which are a good thing – trump higher doses of Lipitor in preventing heart disease. But can adequate levels of “good” cholesterol also counterbalance the cardiovascular risk when “bad”cholesterol levels are high?
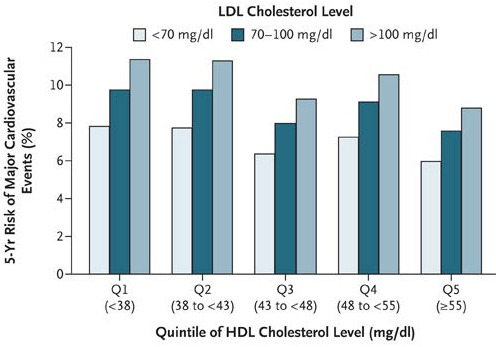
In a word, yes. Take a look at Figure 2: as HDL level increased, the risk of a cardiovascular
event decreased. But more surprising, if HDL and LDL levels were both high (above 55 and 100 mg/dL, respectively), a person had nearly equal risk of a major cardiovascular event as someone who had good LDLs (<70 mg/dL) but bad HDLs (<38 mg/dL)!
Similar evidence is mounting that high triglyceride levels are also an independent risk factor for heart disease. In fact, one study showed that even when people with a history of heart problems used statins to lower their LDLs to acceptable levels, slight increases in triglyceride levels significantly increased the chance they'd have another cardiovascular event.
So there is evidence that the other lipids in the blood (HDL and triglycerides) are equally important in predicting heart health. So is it possible to raise your HDL, or lower your triglyceride, levels? You bet. Studies have shown that simple, endurance exercise training significantly decreases triglyceride levels and raises HDL levels in many people.
I'm not saying that diet and exercise changes will work for everyone. But statins shouldn't be viewed as the magic bullet, either. As more studies on the science of exercise emerge, we'll begin to move past the notion that exercise simply burns calories, and deepen our understanding of the complex interactions of physical activity and metabolism.
Can High Blood Glucose Levels Cause Cancer?
Diets high in simple sugars and refined carbs cause metabolic disorders and Type II diabetes in millions of Americans. But to make matters worse, new evidence suggests that high sugar diets may be even more dangerous than we initially thought. Having too much excess sugar in the bloodstream is never a good thing, and can lead to medical complications such as kidney failure, cardiovascular disease, and eye problems. But could high blood sugar also cause cancer? A Swedish research team addressed this question by tracking over 500,000 patients for 10-25 yeas, and published their results in the December issue of PLoS Medicine.
Diets high in simple sugars and refined carbs cause metabolic disorders and Type II diabetes in millions of Americans. But to make matters worse, new evidence suggests that high sugar diets may be even more dangerous than we initially thought. Having too much excess sugar in the bloodstream is never a good thing, and can lead to medical complications such as kidney failure, cardiovascular disease, and eye problems. But could high blood sugar also cause cancer? A Swedish research team addressed this question by tracking over 500,000 patients for 10-25 yeas, and published their results in the December issue of PLoS Medicine.
Similar to the findings of a study conducted in Korea in 2005, the European research team discovered that having elevated blood glucose levels increased the risk of developing certain types cancer later in life, such as pancreatic tumors in women and liver tumors in men. Not only had more cases of cancer occurred when people had high blood sugar, but the chance of survival also plummeted, especially when the person had cervical, espohageal, or colorectal cancers.
The authors present two theories on why elevated blood glucose levels could cause cancer: 1.) high sugar diets may cause an overproduction of insulin or insulin-like growth factor 1 (IGF-1), both of which promote rapid growth of new cells, the catalyzing step to tumor formation. 2.) More glucose in the blood stream could simply be adding fuel to the fire, feeding rogue tumor cells that need lots of energy to run.
Because the studies lacked certain controls, we can't say for sure whether elevated blood glucose levels cause certain tumors to form. For example, the people with high blood glucose levels may have been sedentary, and so the lack of exercise may be what's actually increasing the chances of developing cancer. Regardless, this study gives yet another example of unhealthy lifestyles contributing to comorbidity, a topic discussed at length by Thomas in The Decision Tree book.
What the NYT and Slate Don't Seem to Understand About Behavior Change
Two articles posted online got under my skin this morning, and I just couldn't resist giving my two cents. First, Tara Parker-Pope, of the New York Times says:
Most obesity researchers now agree that metabolic differences, not willpower, are the driving forces behind weight and appetite control. Studies suggest that an imbalance of brain chemicals and hormones, including cortisol, ghrelin, leptin and serotonin, can increase cravings and make certain foods difficult to resist.
Two articles posted online got under my skin this morning, and I just couldn't resist giving my two cents. First, Tara Parker-Pope, of the New York Times says:
Most obesity researchers now agree that metabolic differences, not willpower, are the driving forces behind weight and appetite control. Studies suggest that an imbalance of brain chemicals and hormones, including cortisol, ghrelin, leptin and serotonin, can increase cravings and make certain foods difficult to resist.
Next, Slate's Engber rants:
It's ironic that so many advocates for healthy eating are also outspoken gourmands. Alice Waters, the proprietor of Chez Panisse, calls for a "delicious revolution" of low-fat, low-sugar lunch programs. It's a central dogma of the organic movement that you can be a foodie and a health nut at the same time—that what's real and natural tastes better, anyway. Never mind how much fat and sugar and salt you'll get from a Wabash Cannonball and a slice of pain au levain. Forget that cuisiniers have for centuries been catering to our hedonic hunger—our pleasure-seeking, caveman selves—with a repertoire of batters and sauces. Junk foods are hyperpalatable. Whole Foods is delicious. Doughnuts are a drug; brioche is a treat.
Tara Parker-Pope misses the fact that personal choices (i.e. what she calls 'willpower') directly affect metabolism. Numerous studies have shown that exercise and calorie restriction (aka 'diet') alter the metabolism of our muscle and fat cells, as well as improve cells' resistance to insulin.
High-sugar, high-fat foods are hard to resist no matter who you are. Most of the in-shape people I know have numerous overweight and/or obese relatives. No, these people weren't simply handed the better genes, rather they are in-shape because they constantly bust their ass. They exercise like crazy. At dessert, they pass up the chocolate cake, and take the fruit cup. When they're hungry during the day, they choose a sensible snack as opposed to raiding the company vending machine. These people are not super-heroes. They have spouses and kids. And at the end of a long day they're tired, just like the rest of us. So what keeps them going? Deep down, they know if they stop, they'll just become another statistic. So they pass up that extra half hour of sleep to hit the road for a run at the crack of dawn.
Willpower leads to behavior changes which lead to metabolic alterations; they're not mutually exclusive. Sure, most dieters will never see the drastic results accomplished by participants of 'The Biggest Loser', but Parker-Pope just gave them a reason to not even make the attempt.
As for Engber's article on Slate, he completely overlooks one not-so-little issue: serving size. American fast-food and junk food is packaged in ridiculously-sized (and calorie-laden) servings. I'll bet the farm that the last time you dined at a gourmet restaurant, the waiter didn't ask if you would like to 'Super-Size' your duck confit entree.
Despite my frustration, I agree with Engber on two points: 1.) a fat-tax on sugary beverages and junk food is not the answer to America's health woes, and 2.) such a tax would end up hurting the poor more than anyone else. The differences in price between fresh fruits and vegetables and fast-food/junk-food is really a separate, much larger problem that I'm not going to get into right now.
In both articles, what irks me the most is that we are currently faced with an obesity epidemic. People really don't need to read articles that marginalize the behavior changes that science has shown will make us healthier.