C-reactive Protein: The Good, The Bad, and The Ugly
When something’s wrong with the body, the innate immune system kicks into high gear, sending inflammatory molecules through the body, which help recruit macrophages – the cellular garbage collectors – to the scene. Recent publications show systemic inflammation goes hand-in-hand with cardiovascular disease (CVD) and atherosclerotic vessels. Researchers have been trying to pinpoint which inflammatory markers could potentially be used as biomarkers for CVD risk or progression. Current efforts have zeroed in on one marker in particular, the C-reactive protein, in the hopes of finding a way to assess a person’s risk for CVD both non-invasively and well before a cardiovascular event occurs. Preliminary evidence has shown that in the normal population, the higher the C-reactive protein level, the higher the risk for CVD. But what exactly is a normal population? These days, a full serving of heart disease often comes with a heaping side of Type II diabetes, rheumatoid arthritis, or chronic kidney disease, creating a so-called “co-morbidity” of chronic diseases. Not surprisingly, these secondary disease states also affect the levels of C-reactive protein in the blood. So when a patient has more than one chronic condition, how useful is measuring the C-reactive protein level in predicting CVD risk?
When something’s wrong with the body, the innate immune system kicks into high gear, sending inflammatory molecules through the body, which help recruit macrophages – the cellular garbage collectors – to the scene. Recent publications show systemic inflammation goes hand-in-hand with cardiovascular disease (CVD) and atherosclerotic vessels. Researchers have been trying to pinpoint which inflammatory markers could potentially be used as biomarkers for CVD risk or progression. Current efforts have zeroed in on one marker in particular, the C-reactive protein, in the hopes of finding a way to assess a person’s risk for CVD both non-invasively and well before a cardiovascular event occurs. Preliminary evidence has shown that in the normal population, the higher the C-reactive protein level, the higher the risk for CVD. But what exactly is a normal population? These days, a full serving of heart disease often comes with a heaping side of Type II diabetes, rheumatoid arthritis, or chronic kidney disease, creating a so-called “co-morbidity” of chronic diseases. Not surprisingly, these secondary disease states also affect the levels of C-reactive protein in the blood. So when a patient has more than one chronic condition, how useful is measuring the C-reactive protein level in predicting CVD risk?
A new study published this week in PLoS One by a group at Kings College, London, took a look at people with rheumatoid arthritis (RA), an inflammatory joint condition that also coincides with remarkably elevated C-reactive protein levels. According to the authors, along with swollen joints, sufferers of rheumatoid arthritis are also twice as likely to have a heart attack.
The researchers looked at three subclinical measures of CVD: flow mediated dilation (measures endothelial cell function), intima-medial thickness (measures arterial wall thickness), and pulse wave velocity (measures large artery stiffness), in people with RA and healthy control subjects. The RA group was further subdivided into three tiers according to how much C-reactive protein was circulating in the patient’s blood during a baseline reading.
If C-reactive protein was in fact causing CVD in rheumatoid arthritis patients, the subclinical CVD measures should incrementally change as the level of C-reactive protein increases. However, the researchers found that two of the subclinical measures didn’t change at all as the level of C-reactive protein increased in those with rheumatoid arthritis. The third subclinical measure – the flow mediated dilation value, which measures how responsive endothelial cells are – actually improved as C-reactive protein levels rose, suggesting that the protein may offer a protective function in a chronic state of inflammation.
I’m always scouring scientific papers looking for the next great thing in biomarkers. After all, if a simple blood test can tell us who’s at risk for certain diseases, we could make great strides in diagnosis and treatment of affected people. But I think this paper shows that biomarker readings are not so straightforward. In the complicated web of chronic disease we’re now spinning, we need to better understand how cardiovascular disease biomarkers – particularly inflammatory markers -- change when people have more than one chronic medical condition.
http://www.plosone.org/article/info:doi/10.1371/journal.pone.0010242#pone-0010242-t001
The Truth About Cholesterol
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
Second, the LDL value doesn't tell the whole story. After all, some people that have low LDL levels, still develop heart disease. When your doctor orders a standard lipid panel, LDLs are measured along with other lipids, such as high-density lipoprotein (HDL) cholesterol and triglycerides. What role do these other types of lipids play in cardiovascular health?
Let's start with the first question: Do higher doses of the drug really improve outcomes? This idea popped into my mind while reading a recent study in PLoS One that looked at LDL levels in patients diagnosed with familial hypercholesterolemia, a genetic predisposition to high levels of “bad” cholesterol. Caused by specific DNA mutations on a small region of chromosome 19, familial hypercholesterolemia drastically increases the chances that a person will develop heart disease. In fact, studies estimate that 85% of men with this mutation will have a heart attack by the age of 60.
The PLoS study found that only a minority of people with hypercholesterolemia brought their LDL levels down to recommended values, even when using statins. According to the authors, doctors were being too cautious with Lipitor dosing, and felt that higher doses would help patients reach their LDL targets.
Blood....beginning....to....boil.....
I know this isn't the first time I've climbed up on my soapbox saying “more medication is not always the answer”, but I wanted to find proof. Lo and behold, I came across a good study from the New England Journal of Medicine that calculated the risk of a major cardiovascular event depending on whether people were taking low- or high-doses of Lipitor (10 or 80 mg, respectively).
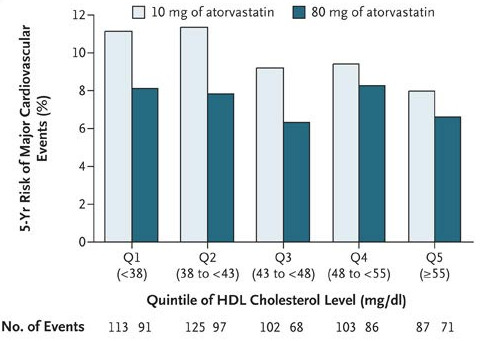
Take a look at Figure 1: Higher doses of Lipitor only made a big difference in risk when HDL levels were low. As HDL levels rose, the difference in height between the light- and dark-green bars went down. This means that if a person can get his or her “good” cholesterol high enough, higher doses of Lipitor will NOT necessarily decrease the risk of having a cardiovascular event.
This finding ties in well with the second question: What role do these other numbers play in cardiovascular health? From the NEJM study, we've seen that high HDL levels – which are a good thing – trump higher doses of Lipitor in preventing heart disease. But can adequate levels of “good” cholesterol also counterbalance the cardiovascular risk when “bad”cholesterol levels are high?
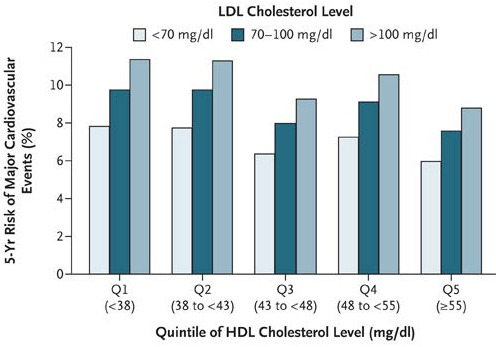
In a word, yes. Take a look at Figure 2: as HDL level increased, the risk of a cardiovascular
event decreased. But more surprising, if HDL and LDL levels were both high (above 55 and 100 mg/dL, respectively), a person had nearly equal risk of a major cardiovascular event as someone who had good LDLs (<70 mg/dL) but bad HDLs (<38 mg/dL)!
Similar evidence is mounting that high triglyceride levels are also an independent risk factor for heart disease. In fact, one study showed that even when people with a history of heart problems used statins to lower their LDLs to acceptable levels, slight increases in triglyceride levels significantly increased the chance they'd have another cardiovascular event.
So there is evidence that the other lipids in the blood (HDL and triglycerides) are equally important in predicting heart health. So is it possible to raise your HDL, or lower your triglyceride, levels? You bet. Studies have shown that simple, endurance exercise training significantly decreases triglyceride levels and raises HDL levels in many people.
I'm not saying that diet and exercise changes will work for everyone. But statins shouldn't be viewed as the magic bullet, either. As more studies on the science of exercise emerge, we'll begin to move past the notion that exercise simply burns calories, and deepen our understanding of the complex interactions of physical activity and metabolism.
A Microbial Census
One morning, a little over a year ago, I woke up with a very sore, and slightly swollen elbow. I remembered that I had cut my arm on a neighborhood bar table while watching a football game with some friends a few days prior, and I wondered if the cut was infected. I made an appointment with my primary care physician, who quickly diagnosed me with bursitis, an inflammation of the fluid-filled sac that pads the elbow. Since I had broken skin, the doctor wisely prescribed clindamycin, an antibiotic, to treat any tissue infection that may have seeped in. As the hours crept by, the pain in my elbow worsened, until I woke up in the middle of the night with extreme arm pain. I immediately checked the elbow that had been swollen the previous day. The swelling had doubled in size, and the skin was an angry-red color. The following morning, I was back in the clinic, and my doctor started to suspect that this was no ordinary infection on my elbow, and may in fact be a drug-resistant staph infection. Gulp. Nonetheless, he felt confident that the clindamycin should clear it up.
One morning, a little over a year ago, I woke up with a very sore, and slightly swollen elbow. I remembered that I had cut my arm on a neighborhood bar table while watching a football game with some friends a few days prior, and I wondered if the cut was infected. I made an appointment with my primary care physician, who quickly diagnosed me with bursitis, an inflammation of the fluid-filled sac that pads the elbow. Since I had broken skin, the doctor wisely prescribed clindamycin, an antibiotic, to treat any tissue infection that may have seeped in. As the hours crept by, the pain in my elbow worsened, until I woke up in the middle of the night with extreme arm pain. I immediately checked the elbow that had been swollen the previous day. The swelling had doubled in size, and the skin was an angry-red color. The following morning, I was back in the clinic, and my doctor started to suspect that this was no ordinary infection on my elbow, and may in fact be a drug-resistant staph infection. Gulp. Nonetheless, he felt confident that the clindamycin should clear it up.
Under the doctor's orders, I spent the next day meticulously tracing the swollen area on my elbow with a Sharpie marker, carefully noting how much it spread. By the end of the day, my entire forearm was puffy and discolored, and my doctor said it was time for me to be admitted to the hospital. I spent 3 days there, getting intravenous treatments of vein-burning, gastrointestinal-rearranging Vancomycin pumped into my system. Not fun.
Afterward, I talked to a number of physician friends about my experience. They said my doctor's treatment plan was textbook. He had done everything right. When docs suspect drug-resistant staph, the first line of defense is typically a hearty dose of clindamycin. The problem in my case was that the staph I contracted was actually resistant to clindamycin. That explains why the infection continued to spread even though I was taking the antibiotics.
Since this little microbial foray, I've had a growing interest in infectious disease. Specifically, I like seeing smart, new ways to keep tabs on how bacterium move from place to place. I wonder, if my doctor had known that clindamycin-resistant staph was infiltrating San Francisco, would I have initially received a different antibiotic? In my opinion, this was a clear case where having more data would have aided the diagnosis, and hastened a healthy outcome.
As Thomas pointed out at The Huffington Post, the true promise of personalized medicine is more about data than specialty drugs. Data can be our personal metrics, such as blood pressure, glucose levels, or cholesterol values. But keeping medical data to ourselves would be somewhat shortsighted. The internet has taught us the power of sharing data. We share our photos on Flickr. We share our status messages on Facebook. We share links on Twitter. Likewise, we can share our health and medical data, enabling pooled statistics from large populations. In the case of infectious disease, the best preventive strategy is to know exactly what strains you're up against, and how the microbes are moving into different geographic regions over time.
Researchers recently confirmed the power of sharing microbial data in a new report, published this month in PLoS Medicine. Roughly 25% of us walk around with staph on our skin, yet not all of us get sick. That's because there's relatively few strains that cause serious symptoms. These so-called virulent strains are the ones docs want to track.
Following both methycilin-resistant (MRSA) and methycilin-susceptible (MSSA) staph strains through Europe, the authors coordinated the participation of 450 hospitals in 26 European countries, a logistic feat in its own right. When a case of staphylococcus aureus was found, the bacterium was genotyped (i.e. its DNA was analyzed to identify which strain it came from), and its location recorded. After collecting all the data, researchers could see how a particular strain of staph localized in different geographic regions. For instance, did the virulent strains stay in one hospital, or had they spread throughout the community?
The authors found that most virulent MRSA strains were contained in a health care clinic, meaning that drug-resistant staph was simply hopping from person-to-person within the hospital walls. Occasionally, that MRSA strain would show up at a different, nearby hospital, and rapidly spread in admitted patients. This implies that the carriers of the virulent MRSA strains are patients who are repeatedly admitted to different regional hospitals.
I'll leave you with a final thought: tracking microbes isn't just a task for researchers. In fact, DIYBio types should check out a cool new project called BioWeatherMap, which asks volunteers to swab commonly used public surfaces, such as door knobs or crosswalk buttons, to track pending microbial storm fronts.
Finding the FDA's Drug Safety Information Online
A smart post by The Sunlight Foundation's Nancy Watzman has me thinking about what it really means to have access to all of our personal health data. In the past, I've myopically viewed personal health data as anything that my body produced, in one way or another, and now sits in my shadowy file at the doctor's office. Things like X-rays, MRIs, and blood test results. No doubt, I should have access to all of this information. What about prescription medication? Sure, I can easily make a list of the meds I'm currently taking, or get my doctor to hand this list over if memory fails me. But how much do I really know about these drugs? Most people, myself included, take our doctor's word when he or she decides to put us on a commonly prescribed medications. For example, let's say a patient has blood-work that shows elevated LDL cholesterol on two consecutive screenings, comes from a family where cardiovascular disease runs rampant, and was previously unable to regulate cholesterol levels with strict diet and exercise regimes. If the doctor prescribed Lipitor to treat the problem, a patient may not even think twice about taking it. After all, we see commercials for such drugs on our TV, and we flip past their ads in our magazines. Direct-to-consumer marketing by pharmaceutical companies makes drugs familiar and, presumably, safe.
A smart post by The Sunlight Foundation's Nancy Watzman has me thinking about what it really means to have access to all of our personal health data. In the past, I've myopically viewed personal health data as anything that my body produced, in one way or another, and now sits in my shadowy file at the doctor's office. Things like X-rays, MRIs, and blood test results. No doubt, I should have access to all of this information. What about prescription medication? Sure, I can easily make a list of the meds I'm currently taking, or get my doctor to hand this list over if memory fails me. But how much do I really know about these drugs? Most people, myself included, take our doctor's word when he or she decides to put us on a commonly prescribed medications. For example, let's say a patient has blood-work that shows elevated LDL cholesterol on two consecutive screenings, comes from a family where cardiovascular disease runs rampant, and was previously unable to regulate cholesterol levels with strict diet and exercise regimes. If the doctor prescribed Lipitor to treat the problem, a patient may not even think twice about taking it. After all, we see commercials for such drugs on our TV, and we flip past their ads in our magazines. Direct-to-consumer marketing by pharmaceutical companies makes drugs familiar and, presumably, safe.
But regardless of what advertisements say, the FDA is ultimately responsible for giving drugs the safety stamp of approval. The decision to approve a drug is based on substantial amounts of preclinical (testing in animals) and clinical (testing in humans) data submitted to the FDA by the drug manufacturer.
Let's say someone – a doctor, a patient, a concerned citizen – wants to review the data that the FDA uses to approve a drug. If the drug you're taking was approved after 1998, you can find the FDA's review documents online. If you're prescribed an older medicine, you may strike out when trying to find what the FDA has to say about it. The government's information on drugs approved through 1997 may be released if someone makes a request through the Freedom of Information Act, but the FDA reserves the right to not publish reports if the agency deems the preserved documents are of “poor quality”. In fact, Watzman found that online safety information is missing for 9 of the 25 most commonly prescribed drugs.
For older and newer drugs alike, when the FDA publishes a review online, it's never in a text-searchable format. Rather, the agency prints the original paperwork, edits with white-out to cover “propriety information”, scans the newly edited document, and finally, posts the altered PDFs online.
Are these edited documents, with words covered with white-out and entire sections omitted, really providing us with useful information? Somewhere along the drug approval process, there has to be a succinct memo that circulates around the FDA headquarters describing the agency's major findings on a particular drug. Why can't the FDA publish a simple summary of their findings?
Skeptics may argue that detailed information about a drug already published by pharmaceutical companies in medical journals, such as the New England Journal of Medicine (NEJM) or the Journal of the American Medical Association (JAMA), should suffice. However, there are two problems with the information reported in medical journals. First, most of these journals are not open access, meaning the average consumer cannot access them without paying for the article. Second, many drug companies only publish positive findings, and bury negative results that show less than desirable efficacy or safety.
Watzman's report is an eye-opening look at what's wrong with the flow of drug information as it goes from pharmaceutical company to the FDA to the consumer. If pharmaceutical companies are allowed to market directly to consumers, we should demand the right to know what the FDA has to say about the safety of these drugs.