What Weight Watchers Can Teach Us About Health
I recently spoke with Workforce about what Weight Watchers can teach us about health and what employers need to learn in order to change employees' health behaviors.
I recently spoke with Workforce about what Weight Watchers can teach us about health and what employers need to learn in order to change employees' health behaviors.
“Behavior change is the biggest opportunity that we have, but also the biggest challenge. It’s such a juicy target, but people aren’t so easy to cajole. But I believe that, just because it’s hard, it doesn’t mean that we shouldn’t keep trying.”
We also chatted about visualizing health data, Flip the Clinic (more on that soon), Iodine, and my role as Entrepreneur in Residence at RWJF.
Thanks to Workforce's Rita Pyrillis for the in-depth profile.
Behavior Change, On the Road
It’s my first trip to London, or to the UK for that matter. The city itself has the distinctive, quintessential, old-world charm I pictured, yet it’s blanketed with the expected conveniences of modern technology. My office for the past two days has rotated between a few wifi-enabled local pubs, a scene that may in fact be the clearest example of the integration of the old and the new. Some simple trip stats thus far: Days in London: two. Number of times I’ve ordered fish and chips as a meal: two. Number of close calls I’ve had with speeding cars after looking in the wrong direction while crossing the street: four (This is in spite of the clearly marked ‘Look Left’ or ‘Look Right’ warnings pasted in the crosswalk).

It’s my first trip to London, or to the UK for that matter. The city itself has the distinctive, quintessential, old-world charm I pictured, yet it’s blanketed with the expected conveniences of modern technology. My office for the past two days has rotated between a few wifi-enabled local pubs, a scene that may in fact be the clearest example of the integration of the old and the new. Some simple trip stats thus far: Days in London: two. Number of times I’ve ordered fish and chips as a meal: two. Number of close calls I’ve had with speeding cars after looking in the wrong direction while crossing the street: four (This is in spite of the clearly marked ‘Look Left’ or ‘Look Right’ warnings pasted in the crosswalk).
Being born on the east coast, and having frequent access to the hustle and bustle of New York City, the past four years in laid-back San Francisco has redefined my view of city life. But London makes San Francisco look like a city of hardasses. Here, everything is toned down a bit. Even the beer is easygoing. An IPA in California will knock your socks off with its alcohol content (some of them upward of 7% ethanol), and bowl you over with the bitter taste of hops. But here the IPA is actually an enjoyable experience for most, smooth and mellow.
If I ever did a stint living overseas, I think I’ve found my city.
Indeed, the past two weeks have been insane as we took PLoS Blogs from a pipe dream to a fully-functional website. Lack of sleep, not eating properly, and the constant adrenaline rush that follows building the next great science communication platform definitely took its toll on me. I still got a fair amount of running in these past days, but nothing fast, nothing crazy.
Following the stress of the past few days and the abundance of fish and chips in my belly, going for a run was the number one priority for today. I opted, however, for a much safer treadmill jaunt rather than navigating the city streets and traffic patterns that flat out confuse me. I only intended to get a quick 3- or 4-miler in, because I had a great deal of work to do, and was still trying to slay the seemingly insurmountable jet-lag beast.
But today’s run was easier than expected, if not easier than usual. Instead of an obligatory run where I count off the seconds until I’m done, I had to force myself to stop after nearly 6-miles. Why was it so much easier today? More than likely, the difference was all in my head. Was I still caught in the adrenaline rush that preceded the launch of PLoS Blogs? Was I still riding the dopamine wave from our success and the congratulatory emails? Perhaps. But the difference may have also, at least in part, been due to the equipment itself.
When I run, there’s no doubt a small dopamine burst somewhere in my head every time I hit another mile marker. There’s just something about whole numbers that resonates with my reward system. With the mileage tracked in kilometers, those dopamine bursts occurred more frequently, which may help explain the increased enjoyment of today’s run.
Another feature of this treadmill was its display, which charted your progress around an outdoor course or circumnavigating a 400m track. For me, watching a small red dot hop along this computer-generated scenery certainly tops either blankly staring at a wall or even watching TV while using a treadmill.
Both Thomas and I have written before on this blog about how technology can change behaviors. And admittedly, I’ve often blindly thought that change means initiating new behaviors. But today, technology also seemed to help me keep those behaviors going longer than usual, an equally important aspect to healthy living.
While my scientific “study” (playing it fast and loose with the word “study”, I know) is riddled with holes and confounders, it’s compelling to think about the consequences of small rewards in behavior change.
When I get back to reality, I’ll see if I can dig up some scientific studies on this idea. But for now, I’m off to a pub with some friends.
Cheers.
photo via Flickr/anirudh koul
Time to Make a Dopamine Run
It's 6am and my alarm clock is buzzing, but I don't hear it. I don't even move. But the incessant noise wakes my wife, and her gentle nudges (read: elbows) and soft whispers (read: expletives) eventually convince me to get out of bed. It seemed like a great idea: Run in the morning before work, to free up countless evening hours. “Think of all you'll get done at night if you don't have to run after work”, I said to myself. “For once you'll actually hit your goal of blogging multiple posts per week! Maybe even finish some of those half-read books lining the shelves.” But two days into the new regime, I'm having second thoughts.
It's 6am and my alarm clock is buzzing, but I don't hear it. I don't even move. But the incessant noise wakes my wife, and her gentle nudges (read: elbows) and soft whispers (read: expletives) eventually convince me to get out of bed. It seemed like a great idea: Run in the morning before work, to free up countless evening hours. “Think of all you'll get done at night if you don't have to run after work”, I said to myself. “For once you'll actually hit your goal of blogging multiple posts per week! Maybe even finish some of those half-read books lining the shelves.” But two days into the new regime, I'm having second thoughts.
It's freaking early. I mean, I've gotten up at the crack of dawn to work on blog posts, but going out for a 6-mile run requires a bit more activation energy than typing away on the computer.
To make matters worse, I just don't feel like running today. It's cold and raining. I can hear the wind blowing from inside my apartment. My warm bed is calling to me, but I muster the will to put on my running clothes, and step outside.
I trod along, slower than usual, because my legs are still tight. A few minutes into the workout, a homeless man approaches me on a rickety bike. He rides close by, taunting me. “You keep running, boy”, he says. “Gonna run yourself right into the grave!” Living in San Francisco, I’ve grown moderately accustomed to such neighborhood friends. But today, instead of being a minor annoyance I shrug off, this guy truly sounds like the voice of reason.
We talk a lot on this blog about ways to drive healthy behavior change: Self-tracking and the Hawthorne effect. Competition and group dynamics. But no way around it, rewards are the heart of behavior change, thanks to the way our brains respond to the molecule dopamine, which differentiates what you have to do, from what you want to do. Dopamine turns a chore into a hobby.
The clearest example of the dopamine reward system in action is the now-famous experiments of Ivan Pavlov. In the early 1900’s, Pavlov noticed that when dogs saw food coming, they began to salivate. The dog's brains were moving faster than their bodies, already anticipating the sweet reward of food before a morsel even hit their mouths. So Pavlov wondered what would happen when he paired a food reward with a random stimulus, such as a bell, whistle, or electric shock. We all know how the story ends: After training, Pavlov's dogs salivated when they heard they bell, regardless if they got a food reward or not.
Pavlov's experiment unlocked our understanding of classical conditioning: Pair a random stimulus close enough to a reward, and soon the stimulus itself tells the brain to get ready for the big payout.
With brains wired for immediate reward in a world of instant gratification, it’s easy to see why we struggle when starting a new exercise routine. The stimulus (the act of running) is so far separated from the reward (the endorphin kick, the runner’s high, or even improvements in our health and fitness).
So how can we ever be expected to change a behavior unless we get an instant payout for our actions? A hand-waiving explanation would be we’ve simply trained our brains to wait longer and longer for the reward. On the other hand, consider this: If you talk to enough runners, they'll tell you they don't “feel right” when they haven’t gone for a run in a few days. They feel “off” if they don’t get their fix. I’m certainly not the first to wonder if chronic exercise somehow primes the dopamine reward system to make us crave the activity, the old “exercise addiction” theory. But the similarities between the two are striking. Could we one day use what we know about addiction to drugs to reveal new ways to get people hooked on positive behavior changes? I’m still funneling through the scientific literature regarding exercise addiction, so I’ll give you updates as the ideas surface.
For any new runners out there looking for pearls of wisdom about what to do when the going gets tough, I leave you with this: I know that even experienced runners lack motivation at times. In fact, I don't know that it ever gets easier to plunge into the first few steps of a run on days you’re dealing with bad weather, a busy schedule, or belligerent guys on bikes. But hang in there, your body and brain will thank you (hopefullly sooner than) later.
What Did the NIH Report on Lifestyle Modification/Alzheimer's Really Say?
My inbox flooded with links to the report released by NIH (and evangelized by TIME) stating that lifestyle interventions (diet, physical activity, mental exercises, etc.) may not be that effective in preventing Alzheimer's Disease. Before I mount my full counterattack, I need to carefully read through the studies the meta-analysis cites. Still, a quick glance at the exclusion criteria of the meta-analysis reveals the authors limited their review to studies using patients over the age of fifty. So really, these results imply that lifestyle modifications may not prevent, delay, or treat Alzheimer's Disease if you start these changes later in life.
My inbox flooded with links to the report released by NIH (and evangelized by TIME) stating that lifestyle interventions (diet, physical activity, mental exercises, etc.) may not be that effective in preventing Alzheimer's Disease. Before I mount my full counterattack, I need to carefully read through the studies the meta-analysis cites. Still, a quick glance at the exclusion criteria of the meta-analysis reveals the authors limited their review to studies using patients over the age of fifty. So really, these results imply that lifestyle modifications may not prevent, delay, or treat Alzheimer's Disease if you start these changes later in life.
My second point is that all lifestyle modifications are not created equal. Scientific evidence in animal studies suggests that of all interventions, aerobic exercise is our best chance of staving off cognitive decline. In fact, this meta-analysis also found some correlation between exercise and preserving or improving cognitive ability.
There's a good article in The Economist that discusses the failures of the drug industry to find a solution to treating Alzheimer's Disease. One particular quote resonates with my feelings on the NIH report:
Another fundamental problem is that, whatever is causing the damage, treatment is starting too late. By the time someone presents behavioural symptoms, such as forgetfulness, his brain is already in a significant state of disrepair. Even a “cure” is unlikely to restore lost function.
The Truth About Cholesterol
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
Second, the LDL value doesn't tell the whole story. After all, some people that have low LDL levels, still develop heart disease. When your doctor orders a standard lipid panel, LDLs are measured along with other lipids, such as high-density lipoprotein (HDL) cholesterol and triglycerides. What role do these other types of lipids play in cardiovascular health?
Let's start with the first question: Do higher doses of the drug really improve outcomes? This idea popped into my mind while reading a recent study in PLoS One that looked at LDL levels in patients diagnosed with familial hypercholesterolemia, a genetic predisposition to high levels of “bad” cholesterol. Caused by specific DNA mutations on a small region of chromosome 19, familial hypercholesterolemia drastically increases the chances that a person will develop heart disease. In fact, studies estimate that 85% of men with this mutation will have a heart attack by the age of 60.
The PLoS study found that only a minority of people with hypercholesterolemia brought their LDL levels down to recommended values, even when using statins. According to the authors, doctors were being too cautious with Lipitor dosing, and felt that higher doses would help patients reach their LDL targets.
Blood....beginning....to....boil.....
I know this isn't the first time I've climbed up on my soapbox saying “more medication is not always the answer”, but I wanted to find proof. Lo and behold, I came across a good study from the New England Journal of Medicine that calculated the risk of a major cardiovascular event depending on whether people were taking low- or high-doses of Lipitor (10 or 80 mg, respectively).
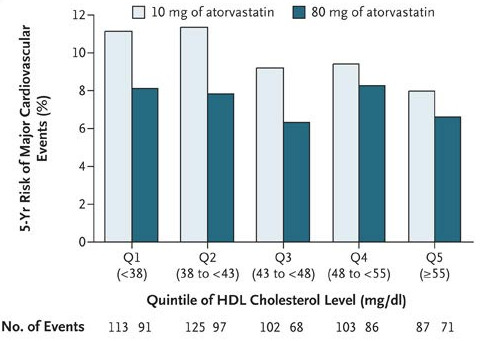
Take a look at Figure 1: Higher doses of Lipitor only made a big difference in risk when HDL levels were low. As HDL levels rose, the difference in height between the light- and dark-green bars went down. This means that if a person can get his or her “good” cholesterol high enough, higher doses of Lipitor will NOT necessarily decrease the risk of having a cardiovascular event.
This finding ties in well with the second question: What role do these other numbers play in cardiovascular health? From the NEJM study, we've seen that high HDL levels – which are a good thing – trump higher doses of Lipitor in preventing heart disease. But can adequate levels of “good” cholesterol also counterbalance the cardiovascular risk when “bad”cholesterol levels are high?
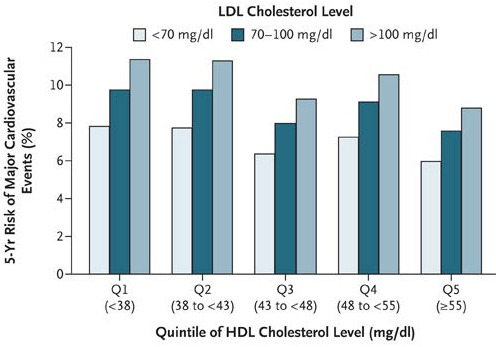
In a word, yes. Take a look at Figure 2: as HDL level increased, the risk of a cardiovascular
event decreased. But more surprising, if HDL and LDL levels were both high (above 55 and 100 mg/dL, respectively), a person had nearly equal risk of a major cardiovascular event as someone who had good LDLs (<70 mg/dL) but bad HDLs (<38 mg/dL)!
Similar evidence is mounting that high triglyceride levels are also an independent risk factor for heart disease. In fact, one study showed that even when people with a history of heart problems used statins to lower their LDLs to acceptable levels, slight increases in triglyceride levels significantly increased the chance they'd have another cardiovascular event.
So there is evidence that the other lipids in the blood (HDL and triglycerides) are equally important in predicting heart health. So is it possible to raise your HDL, or lower your triglyceride, levels? You bet. Studies have shown that simple, endurance exercise training significantly decreases triglyceride levels and raises HDL levels in many people.
I'm not saying that diet and exercise changes will work for everyone. But statins shouldn't be viewed as the magic bullet, either. As more studies on the science of exercise emerge, we'll begin to move past the notion that exercise simply burns calories, and deepen our understanding of the complex interactions of physical activity and metabolism.
How "The Science of Success" Redefines Psychology
I just finished reading Dave Dobbs' new article in the the December issue of The Atlantic, "The Science of Success". Dobbs turns the classic question of Nature vs. Nurture, whether our genes or our environment are the deterministic drivers of our fate, on its head. Traditionally, those who support "nature" say that our genes are most influential in defining us. On the other hand, those that support the "nurture" side say that our environment plays a more important role. Based on new research, Dobbs introduces the idea of two types of people, "dandelions" and "orchids". Dandelions can thrive anywhere, despite their environment or upbringing. Orchids, however, are more temperamental, and require a stable environment to survive. At first glance, the orchids may seem like a liability, and in fact, they often carry genes that make them susceptible to mood disorders and psychological disease. The astounding part of Dobbs' report is that he shows that given the right care, or environment, the orchids don't just do OK, but far surpass the dandelions in perfomance. In other words, given the right training, orchids may in fact be destined for greatness.
I just finished reading Dave Dobbs' new article in the the December issue of The Atlantic, "The Science of Success". Dobbs turns the classic question of Nature vs. Nurture, whether our genes or our environment are the deterministic drivers of our fate, on its head. Traditionally, those who support "nature" say that our genes are most influential in defining us. On the other hand, those that support the "nurture" side say that our environment plays a more important role. Based on new research, Dobbs introduces the idea of two types of people, "dandelions" and "orchids". Dandelions can thrive anywhere, despite their environment or upbringing. Orchids, however, are more temperamental, and require a stable environment to survive. At first glance, the orchids may seem like a liability, and in fact, they often carry genes that make them susceptible to mood disorders and psychological disease. The astounding part of Dobbs' report is that he shows that given the right care, or environment, the orchids don't just do OK, but far surpass the dandelions in perfomance. In other words, given the right training, orchids may in fact be destined for greatness.
This finding redefines conditions we typically may have classified as undesirable. ADHD, depression, and generalized anxiety disorder, are no longer conditions to dread, because given the right training, people with these predispositions may in fact be the true "movers and shakers" in the world.
Please read the full article for yourself. And, as always, I'd welcome a discussion here...
Why Behavior Change Is (Still) Better Medicine Than Drugs
While attending the Institute for the Future's Health Horizons Fall Conference on Monday, one thing became eminently clear. The 21st century will be the era of brain, the last great scientific frontier. Due to societal shifts, environmental changes, and the fact that we are just living longer, we are poised to see a sharp rise in cases of diseases such as Alzheimer's, Parkinson's, autism, and post-traumatic stress disorder. The only thing worse than the increasing prevalence of brain disease is the sobering fact that few viable treatments currently exist.

While attending the Institute for the Future's Health Horizons Fall Conference on Monday, one thing became eminently clear. The 21st century will be the era of brain, the last great scientific frontier. Due to societal shifts, environmental changes, and the fact that we are just living longer, we are poised to see a sharp rise in cases of diseases such as Alzheimer's, Parkinson's, autism, and post-traumatic stress disorder. The only thing worse than the increasing prevalence of brain disease is the sobering fact that few viable treatments currently exist.
For years, we've heard the mantra of behavior change and health. Exercise more and you'll cut your risk for heart disease and stroke. Eat more fruits and vegetables and you can decrease your risk for colon cancer (or possibly prostate cancer, as discussed in a previous Decision Tree post, "Why Behavior Change is Better Medicine than Drugs"). Could behavior change serve our brain health as well as it did other organs of the body?
On Monday, the neurotechnology community drew a definitive line in the sand with regard to treating the brain. On one side were panelists that believed that society is not being medicated enough for mental disorders, including ADHD in children. On the other side, proponents of behavioral training argued that brain plasticity, the innate ability of the brain to rewire itself continuously throughout life, is our best bet to combat brain disease.
Consider the use of ADHD drugs in children, or cognitive-enhancing drugs, such as modafinil, by professionals (including a large group of scientists) in the workplace. Proponents of medication say that the cognitive enhancers are not doing anything unnatural. Rather, they are taking someone who's a mediocre performer in terms of concentration, and simply moving them to the upper 90th percentile. Then, according to the same logic, I guess these panelists would also support legalizing steroids in major league baseball. After all, the steroids are not making the athletes super-human. Rather, they're taking the middle-of-the-road performers and nudging them to the upper echelon of the sport. Hmmm....
My former postdoc advisor, Dr. Michael Merzenich of the University of California San Francisco, led the charge for behavioral training as a better alternative to drugs for diseases of the brain. Mike's lifelong work focused on the neuroscience of learning, and how brain plasticity occurs at various stages of development. He believes that many ailments of the brain, including ADHD, occur because we are using our brains "incorrectly", but specific behavioral training can reverse and improve these deficits.
The wonders of behavioral training and brain plasticity are not limited to sparse findings in a dark lab. In fact, Mike's most promising research has been translated into several commercial computer software applications, which have enhanced the reading capabilities of dyslexic children, as well as improved the speech processing and memory of senior citizens.
Whether you are sold on behavioral training as a feasible alternative to drug therapy in brain illness or not, one point remains solid: the cost of conducting clinical trials for behavioral training regiments is a mere fraction of the cost of drug trials. Given that it's terribly expensive to run drug trials, and that only a small fraction of drugs in a pharma company's pipeline succeeds in the clinic, we clearly can't afford to ignore behavioral training as a new way to treat the brain.
How Much Personal Data is Needed to Stay Healthy?
A few months ago, a story ran in Wired Magazine that described a noticeable shift in the scientific method, and attributed the change to our ability to produce and store large amounts of data.Historically, the scientific method was built around a testable theory. But in the 21st century, theories were becoming obsolete; the data simply spoke for itself.
A few months ago, a story ran in Wired Magazine that described a noticeable shift in the scientific method, and attributed the change to our ability to produce and store large amounts of data.Historically, the scientific method was built around a testable theory. But in the 21st century, theories were becoming obsolete; the data simply spoke for itself.
Data from our bodies is no exception -- physiologic data can now be accessed as a real-time data stream thanks to personal health monitors. But does the vast amount of data we get from our bodies make us any healthier? Do we need to collect data 24-hours a day in order to learn something interesting about our health? Is it even feasible to wear these sensors all day, every day?
I am embarking on a new self-tracking experiment to answer these questions (and possibly a few others). For 30 days, I will be using devices such as the Zeo personal sleep coach, the Philips DirectLife activity monitor, the Mio Motiva wristband on-demand heart rate monitor, and the Nike+ sportband. The goal of this study is not to pit one device against another; rather, I want to focus on what the data tells me, and how I can best use it to stay healthy.
I'll get a blog post up here at least once a week, all the while working on a longer story about the journey that will be released at the end of the month.
Stay tuned. It should be a fun ride...
The Reward System Actually Reduces Motivation? Really?
I just wanted to offer a rebuttal to the following tweet that popped up on my stream today:
@GuyKawasaki The reward system actually reduces motivation http://om.ly/MHzl
I just wanted to offer a rebuttal to the following tweet that popped up on my stream today:
@GuyKawasaki The reward system actually reduces motivation http://om.ly/MHzl
First, let's take a look at the cited study. The experimental groups were defined as:
The children were then randomly assigned to one of the following conditions:
- Expected reward. In this condition children were told they would get a certificate with a gold seal and ribbon if they took part.
- Surprise reward. In this condition children would receive the same reward as above but, crucially, weren't told about it until after the drawing activity was finished.
- No reward. Children in this condition expected no reward, and didn't receive one.
While reading this study, we have to ask ourselves: Is a "certificate with a gold seal" really a reward? Is that what best motivates children? Do the results of this study conclude that children don't change their behaviors for rewards, or simply that the reward itself was lame?
Despite what the authors state, small rewards CAN be a powerful impetus for behavior change. Reward is a staple of behavioral training, and in particular, rewards that release dopamine (e.g. food, sweet beverages, etc.) strongly influence brain plasticity during a training event. To make a blanket statement on the contrary is dangerous. Preventable disease is a huge drain on our health care system, and it's been shown that simple behavior changes like diet and exercise can reduce the burden caused by obesity, diabetes, and heart disease. Just because a child responds in a certain way to a reward of a certificate with a gold star, I don't think we should abandon the proverbial "carrot" when trying to get people healthy.
Behavior Change: A Central Topic at Health 2.0
The afternoon of Day 1 of the Health 2.0 Conference was highlighted by the session, "The Patient is In". First up, a video that documented the experiences of a group of people that recently started using patient health tools, such as online health journals that track diet or exercise, support sites for quitting smoking, or home blood test kits.

The afternoon of Day 1 of the Health 2.0 Conference was highlighted by the session, "The Patient is In". First up, a video that documented the experiences of a group of people that recently started using patient health tools, such as online health journals that track diet or exercise, support sites for quitting smoking, or home blood test kits.
Following the video, a few of the participants were joined onstage by technology pioneer Esther Dyson. Some panelists said that while they exercised a bit more and ate somewhat better during the course of the experiment, soon after they returned to their old (bad) habits. Others were completely sold on the idea of self-tracking, and one particular panelist said that his daily running and mile-logging inspired his daughter and her friend to do the same. Likewise, his neighbor, having noticed him trotting around the neighborhood several times a week, started his own walking regiment. In the panelist's words, "People draw energy from supportive environments".
Social contagion, the idea that behavior change can be contagious, has been gaining ground. A few months ago, I experienced the power of social contagion for myself: as many readers know, I'm a long-time runner. But no matter how many miles I logged per week, my wife never really understood why I was out on the road, tormenting myself for hours. It wasn't until she bought a Nike+ sensor, and her boss challenged her to a "See Who Can Run More Miles in a Month" challenge that she became hooked on running. Now I have to spy on her website running log to make sure I still run more miles per week (yes, I'm competitive too).
Some people are inspired to change their behaviors by logging how many calories they're consuming every day. Others are motivated by seeing friends or family stop smoking. And for some, it takes someone else to throw down the gauntlet, and say, "I bet I can kick your butt in a race around the track" for the change to occur.
Esther Dyson concluded the session by saying that we can also drive behavior changes by associating the things we just don't like to do with small "rewards". Personally, she rewarded the monotony of flossing with a 5-minute reprieve from her intense exercise routine. So on days she flossed, instead of swimming for an hour, she could quit after 55 minutes.
Social contagion and little rewards go a long way in keeping people focused and motivated, and I was glad to see these ideas brought up at today's conference.