Will Keas Live Up To Its Potential?
"The human body does enormously well healing itself," Keas founder, and ex-Google Health lead, Adam Bosworth told Health 2.0 conference-goers shortly after stepping on stage. On the heels of an article in the New York Times that touted the company's beta launch, Bosworth walked the crowd through the way we'll keep ourselves healthy in the future, using Keas' platform.
"The human body does enormously well healing itself," Keas founder, and ex-Google Health lead, Adam Bosworth told Health 2.0 conference-goers shortly after stepping on stage. On the heels of an article in the New York Times that touted the company's beta launch, Bosworth walked the crowd through the way we'll keep ourselves healthy in the future, using Keas' platform.
Over the past few years, Bosworth carefully watched as the Health 2.0 revolution unfolded. Medical issues became less of a private experience. People, who at one time only discussed personal ailments with their family physician, now turned to family and trusted friends for medical advice. With the boom of the Internet, a person's trusted medical community suddenly became infinite.
Of all people, Bosworth understood the potential power of the internet on health, where the collective wisdom of the patient population could reach thousands, or millions, of other people. So he wondered, if people were readily turning to the web for information when they got sick, could customized, preemptive web advice keep people from getting sick in the first place?
Keas' system uses custom "Care Plans" that collect personal data that the user either uploads at the website, or is transferred directly from a lab, like Quest Diagnotics. Keas plans to run its own iPhone-like App Store, where doctors or other health care providers create their own Care Plans, integrate them into the Keas platform, and instantly distribute them to millions of people.
By personalizing the measures we can take to stave off certain predisposed conditions, Keas' Care Plans should improve our health. But the real promise of the company, wasn't in what Bosworth delivered onstage, but rather, in something he simply mentioned in passing. Bosworth alluded to the idea that not only will Keas' platform let people track their own health, but it could also allow people to keep tabs on their family's health as well.
Imagine logging into your Keas profile, and being presented with a dashboard that shows the current health information for your spouse, child, and elderly parent. Did your husband get his blood work test today? How much has your child exercised? Has your 80-year-old father read the online information packet on "Preventing Falls in the Home"? At a glance, you'd have this information in front of you on the Keas website, if the company follows through with this idea.
When people become chronically ill, or simply start living into their eighties and nineties, maintaining health shifts from an individual to a team sport. There's too much information for one person to process and comprehend. Too many medications. Too many things to keep straight. Current estimates put 30 million people in the US as primary caregivers -- adults, aged 18 or over, who maintain the personal well-being of another adult. Keas' program has the potential to make the term "long-distance caregiver' obsolete. Everyone would be just a click away from checking-in with their loved ones.
Health 2.0 Conference Day 2: Consumer Aggregators
Welcome to Day 2 of the Health 2.0 conference. There was an interesting talk this morning focused on "Consumer Aggregators", which demoed new applications from WebMD, Google Health, and Microsoft Heath Vault.

Welcome to Day 2 of the Health 2.0 conference. There was an interesting talk this morning focused on "Consumer Aggregators", which demoed new applications from WebMD, Google Health, and Microsoft Heath Vault.
Wayne Gattinella of WebMD summarized the state of affairs, saying that people want to access information on the go, and there's a drastic need for medical applications to go mobile. According to Gatinella, this means creating applications for both physicians, in a point-of-care setting, as well as patients, who want on-demand information about their health.
All three companies agreed that people are sharing more and more personal health data online these days. Gattinella paralleled patients sharing their medical information to using credit cards online 10 years ago. At first, people were skeptical and scared. After successfully trying it out a few times, fears subsided, and the convenience benefit far outweighed the perceived risk.
Each application displayed different, but equally cool, themes. Microsoft built their application around the idea that patients should be able to customize the layout as they wanted -- place your blood pressure widget here, your LDL cholesterol level widget over there.
Google Health's application stressed the fact that less than 25% of what a doctor tells a patient during an office visit is actually remembered by that patient when they get home. Google closes this gap in communication in the MDLiveCare application by feeding all of the doctor's notes back into the patient's Google Health record, so that the patient can recap the visit at a later time.
WebMD had a nifty iPhone application with a 'symptom tracker', which launched with of a cartoon-like drawing of a human body (i.e. the "virtual patient"). Sore ankle? Click on the virtual patient's ankle, and you'll be presented with some common symptoms that involve the ankle, such as 'swelling', 'rash', or 'laceration'. As the patient navigates through the menu system and answers questions, their symptoms are further refined until the system figures out what is wrong. Ultimately, the patient is presented with a description of the possible problem, e.g. "Click here for information on ankle sprain", which takes you to the WebMD entry for sprained ankles.
I really liked how the focus of this group was "on-demand" information, and all of the applications were tailored to helping the patient gain control of their medical information. The data is theirs to begin with, let's give them a way to harness it...
Health 2.0 Conference: Clinician-Patient Interaction
The morning session focused on clinician-patient interactions. Executives from Myca, VisionTree, AmericanWell, and ReachMyDoctor, presented their virtual doctors' office visit tools. All of the tools had similar features, such as online scheduling, and the choice of different types of offices visits, such as IM chat or video. Most integrated well with personal health records, so that during an office visit, the physician had access to the patient's medication refill history, or overdue routine preventive medical tests, such as blood-work, prostate screens, or mammograms.
The morning session focused on clinician-patient interactions. Executives from Myca, VisionTree, AmericanWell, and ReachMyDoctor, presented their virtual doctors' office visit tools. All of the tools had similar features, such as online scheduling, and the choice of different types of offices visits, such as IM chat or video. Most integrated well with personal health records, so that during an office visit, the physician had access to the patient's medication refill history, or overdue routine preventive medical tests, such as blood-work, prostate screens, or mammograms.
At the end of the panel discussion, several good questions were asked. People wondered what incentives were in place for physicians and patients to use the system, especially if each doctor was using a different system. Does this mean that the patient will have to log on to two different websites if their general practitioner uses HelloHealth, but their cardiologist uses AmericanWell? The panel responded that each of these web applications was part of a larger central platform. It may be more helpful to think of each web tool as an individual iPhone app. iPhone apps can communicate with each other and run on a single system (phone), so it's possible for these individual web tools to play nicely together in the future. One question I had: where are all of the patient tools that plug into this central platform? Maybe that's tomorrow's talk...
The second session brought out some pretty tough critics of the virtual doctor's office idea. Although these new panelists liked what they were seeing and hearing, at heart, they were still physicians that saw many challenges to using these products in their own practice. A psychiatrist was the first to challenge, saying that good psychotherapy demands face-to-face interactions. I've seen this type of push-back from doctors before while consulting at medical device start-up companies. No matter how transformative or revolutionary the new technology could be, unless doctors can easily integrate the technology into their current practice, the idea may flounder.
Yesterday at the Kaiser HealthCamp Un-Conference, a cool term surfaced -- "minimally disruptive technology" -- which was used to describe an approach to reform health care technology that pushed progress, while not upsetting the status quo, so to speak. Granted, there is a learning curve associated with any new technology, and to implement an idea such as virtual doctors' office visits will require significant infrastructure changes in the medical community.
Will only a fringe group of early adapters use this technology? Is it realistic to think that a majority of doctors will use such a system? Too early to tell, but it wouldn't hurt to get some of the nay-sayers involved with the design while the concept is still in its early stages.
Improving Your Medical Literacy
The ideas behind The Decision Tree, in a sense, focus on ways to create the next-generation patient. This new kind of patient will have to understand the context of their own medical self through a combination of genetics, personal metrics/data, and statistics. Needless to say, understanding one's own medical self will also require an increased medical literacy, where patients understand both their conditions, as well as where they fall within the spectrum of their disease.
The ideas behind The Decision Tree, in a sense, focus on ways to create the next-generation patient. This new kind of patient will have to understand the context of their own medical self through a combination of genetics, personal metrics/data, and statistics. Needless to say, understanding one's own medical self will also require an increased medical literacy, where patients understand both their conditions, as well as where they fall within the spectrum of their disease.
Creating the next-generation patient will inevitably require new tools. Website services, such as PatientsLikeMe, have been a step in the right direction towards increasing patient knowledge by empowering people with general knowledge of their conditions, as well as and providing information of what others in their shoes are experiencing. However, focusing on the patient may only address half of the problem.
MedEncentive, a start-up company founded in 2003, approaches the issue of medical literacy by addressing both players in the problem, the physician and the patient. MedEncentive's product focuses on developing, or even better, redefining, the doctor-patient relationship. A statistic listed on their website states that on an average office visit, the physician will interrupt the patient within seconds of entering the room, while the patient only comprehends a fraction of the information given to them by their doctors. Drawing from my own mixed experiences dealing with physicians – including a recent diagnosis botched 3 times in a week – I could see how this could be true. If a patient had an increased understanding of their conditions, perhaps this interaction would not be so one-sided.
The company's core product is an incentive program for doctors and patients that centers around the exchange of medical information. Doctors who participate in the medical literacy program can earn about 20% more (~$15) per office visit by assigning their patients a "to-do" list. The company mentions some of what this list might include, such as questionnaires which determine how much a patient understands about both their current health status and the conditions they've been diagnosed with, as well as how they would rate their doctor's performance. The patients earn rewards, such as copay reimbursements or health savings account credits, for completing their reading assignments and the questionnaires.
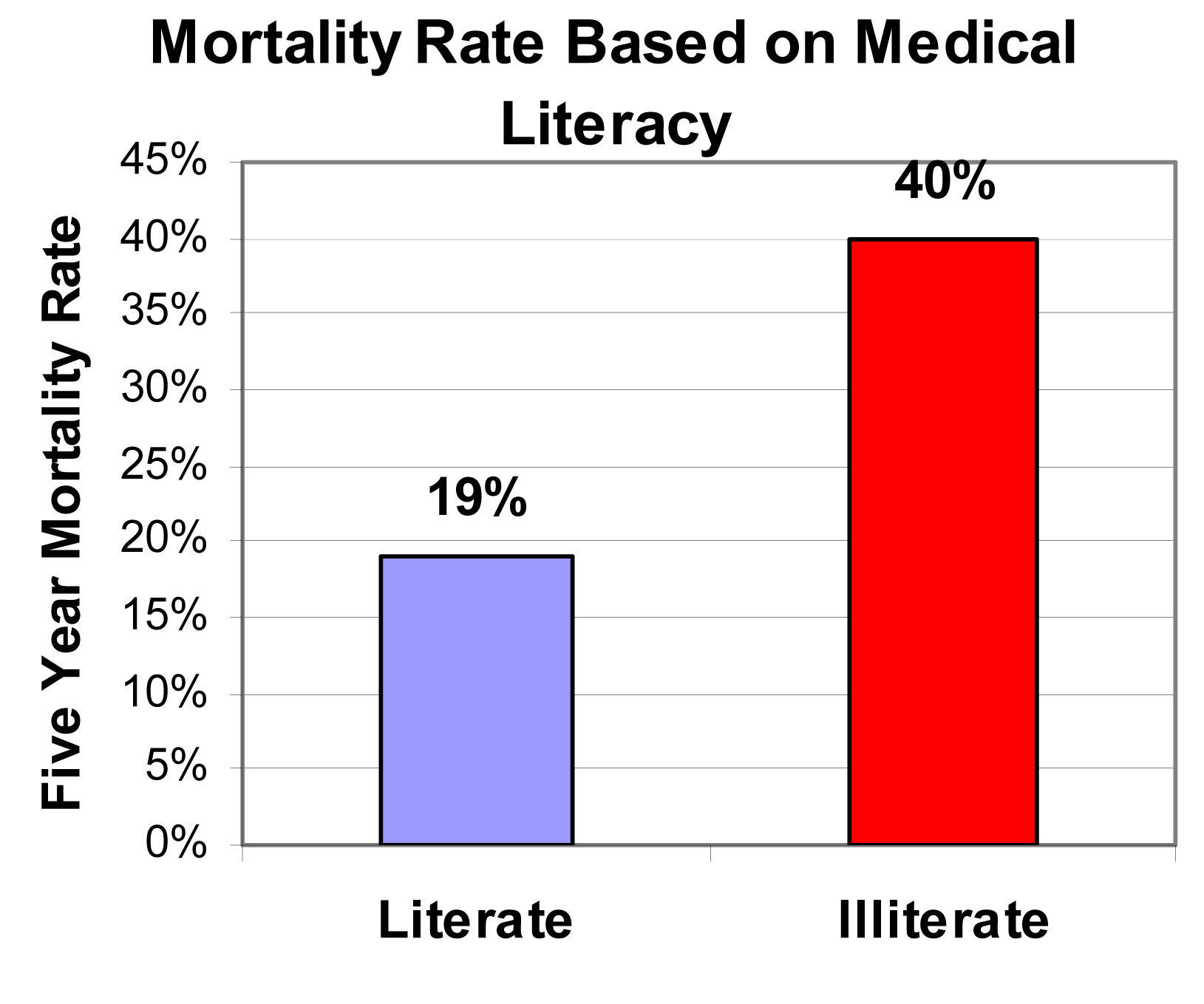
According to the company, a medically literate patient will communicate more efficiently with their physician, while medically illiterate patients will consume more health care resources. But do people really care about this? Sure, it would be nice to reduce health care costs and make doctors and patients best friends, but is it really a big deal if a patient doesn't understand the ins-and-outs of their conditions? If you are not sold on the benefit of developing the doctor-patient relationship, consider the following figure. It was taken from a study conducted by physicians at Northwestern University and Emory University on the 5-year mortality rate of an elderly population. Medical illiteracy can become dangerous when it leads to an increased risk of death. So based on the outcome of this study, MedEncentive's thesis makes sense: when patients know more about their medical conditions, they have better health.
I acknowledge that there is a confounder to this study -- it was conducted in an elderly population. As we all know, the cognitive abilities of the elderly vary drastically across the population. For example, your 90-year old grandfather may be self-sufficient, living on his own, and sharp as a tack, while my 90-year old grandmother requires assisted living. So one question I asked myself when looking at this study was: are the people who are in the medically illiterate group also the ones who are in assisted living? In other words, is the increased risk of death due to the fact that the patient doesn't understand medical jargon, or is it due to an overall decline in their mental capabilities? Luckily, the clinical team already addressed this question. They found that both an increased medical literacy and a higher cognitive ability both independently indicated a longer, healthier life. So those that understand their medical conditions will live longer, but so will those who can still do the New York Times crossword puzzle themselves.
My take: The benefits of medical literacy, as outlined here, are: 1.) knowledge can improve the doctor-patient relationship, and 2.) knowledge can improve health. The Decision Tree is not about a single factor influencing a healthy life, rather it discusses a collective set of behavioral changes that lead to new way to think about and treat disease. I think the results discussed here show that medical literacy is an important piece of the next-generation patient puzzle. In the future, we will be asking a lot from patients, as more of the responsibility for staying healthy will be shifted to them. So I like the approach of MedEncentive to get the doctor involved as well. In the end, what we end up with is the next-generation patient, as well as a new breed of physician -- one who is willing to break the current mold.