Sugar-coated Laziness
Check out this study. Researchers found that when "teenage" rats (30-45 days old) consumed massive amounts of sugar, they became extremely difficult to train as adults. For two weeks or so during adolescence, one group of rats had free access to a tasty 5% sucrose solution, while the control group only had water available. Similar to some American teenagers, the experimental group of rats consumed about 20% of their daily caloric intake as simple sugar.
Check out this study. Researchers found that when "teenage" rats (30-45 days old) consumed massive amounts of sugar, they became extremely difficult to train as adults. For two weeks or so during adolescence, one group of rats had free access to a tasty 5% sucrose solution, while the control group only had water available. Similar to some American teenagers, the experimental group of rats consumed about 20% of their daily caloric intake as simple sugar.
To give you some background, it's extremely easy to train adult rats to perform simple tasks, such as pulling levers or pressing buttons in return for a food reward. However, the researchers couldn't motivate the rats that had consumed large amounts of sugar as teenagers to learn the task. My first reaction while reading this paper was: "Big deal. That group of rats just had sugar overload. It no longer had any real value for them, so there was no incentive to learn the new task".
But here's where the story gets interesting: if you repeat the experiment, but replace the teenage rats with adult rats, you get strikingly different results. When adult rats have free access to a sugary drink for two weeks, they never lose motivation for the sweet reward, and easily learn the new lever-pull task later in life. So it's not that rats are simply sick of the sweet reward, but rather, it seems the sweet drink over-stimulated the reward pathway in the brain during adolescent development, leading to problems with motivation in adulthood.
Were the calories in the sugary drink or the sweet taste to blame for hyper-activating the reward circuits in the brain? To answer this, the authors took another group of teenage rats and gave them free access to a drink flavored with artificial sweetener, which has no calories. These rats were also unmotivated and rather difficult to train later in life, so the authors concluded that the sweet taste, but not the sugar itself, was hyper-activating the brain's reward circuits.
Besides, ahem, crazy neuroscientists writing for health blogs, who cares about lazy rats? Well, the authors argue that a sign of depression in rodents is lack of motivation to perform simple tasks. Given that incidence rates for depression and other psychological illness are increasing in today's society, it's interesting to see how seemingly benign events during adolescence -- a critical time in brain development -- affect the mental state of adult animals.
The Truth About Cholesterol
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
We've all heard the mantra: keep LDL levels – the “bad” cholesterol – down, and the “good” HDL cholesterol up. But thanks in part to the ubiquity of statins, such as Lipitor, which allow us to simply pop a pill to limit LDL production in the body, we've recently adopted tunnel vision when thinking about managing cholesterol. LDL levels are all we seem to care about now, as we strive for lower and lower numbers at each visit to the doctor's office. However, I think we're missing the bigger picture by focusing solely on LDL. First, it's made us reliant on medication to solve a problem that can many times be addressed with changes in diet and exercise regimes. Once someone starts Lipitor treatment, they'll be taking it for life, and if LDL levels don't quite get as low as they should, it's all too easy to solve the problem by increasing the dose. When patients first begin Lipitor treatment, physicians typically prescribe the lowest possible amount, 10mg. However, dosing can go as high as 80mg, which begs the question: Do higher doses of the drug really improve outcomes?
Second, the LDL value doesn't tell the whole story. After all, some people that have low LDL levels, still develop heart disease. When your doctor orders a standard lipid panel, LDLs are measured along with other lipids, such as high-density lipoprotein (HDL) cholesterol and triglycerides. What role do these other types of lipids play in cardiovascular health?
Let's start with the first question: Do higher doses of the drug really improve outcomes? This idea popped into my mind while reading a recent study in PLoS One that looked at LDL levels in patients diagnosed with familial hypercholesterolemia, a genetic predisposition to high levels of “bad” cholesterol. Caused by specific DNA mutations on a small region of chromosome 19, familial hypercholesterolemia drastically increases the chances that a person will develop heart disease. In fact, studies estimate that 85% of men with this mutation will have a heart attack by the age of 60.
The PLoS study found that only a minority of people with hypercholesterolemia brought their LDL levels down to recommended values, even when using statins. According to the authors, doctors were being too cautious with Lipitor dosing, and felt that higher doses would help patients reach their LDL targets.
Blood....beginning....to....boil.....
I know this isn't the first time I've climbed up on my soapbox saying “more medication is not always the answer”, but I wanted to find proof. Lo and behold, I came across a good study from the New England Journal of Medicine that calculated the risk of a major cardiovascular event depending on whether people were taking low- or high-doses of Lipitor (10 or 80 mg, respectively).
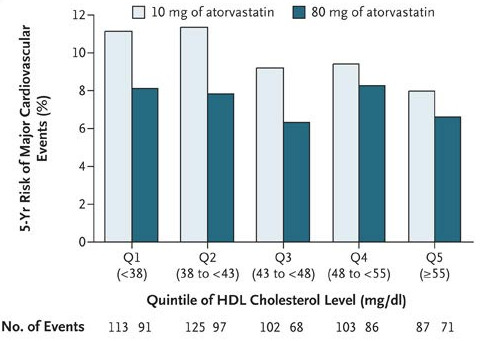
Take a look at Figure 1: Higher doses of Lipitor only made a big difference in risk when HDL levels were low. As HDL levels rose, the difference in height between the light- and dark-green bars went down. This means that if a person can get his or her “good” cholesterol high enough, higher doses of Lipitor will NOT necessarily decrease the risk of having a cardiovascular event.
This finding ties in well with the second question: What role do these other numbers play in cardiovascular health? From the NEJM study, we've seen that high HDL levels – which are a good thing – trump higher doses of Lipitor in preventing heart disease. But can adequate levels of “good” cholesterol also counterbalance the cardiovascular risk when “bad”cholesterol levels are high?
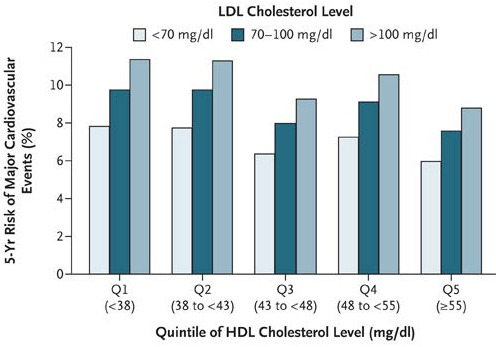
In a word, yes. Take a look at Figure 2: as HDL level increased, the risk of a cardiovascular
event decreased. But more surprising, if HDL and LDL levels were both high (above 55 and 100 mg/dL, respectively), a person had nearly equal risk of a major cardiovascular event as someone who had good LDLs (<70 mg/dL) but bad HDLs (<38 mg/dL)!
Similar evidence is mounting that high triglyceride levels are also an independent risk factor for heart disease. In fact, one study showed that even when people with a history of heart problems used statins to lower their LDLs to acceptable levels, slight increases in triglyceride levels significantly increased the chance they'd have another cardiovascular event.
So there is evidence that the other lipids in the blood (HDL and triglycerides) are equally important in predicting heart health. So is it possible to raise your HDL, or lower your triglyceride, levels? You bet. Studies have shown that simple, endurance exercise training significantly decreases triglyceride levels and raises HDL levels in many people.
I'm not saying that diet and exercise changes will work for everyone. But statins shouldn't be viewed as the magic bullet, either. As more studies on the science of exercise emerge, we'll begin to move past the notion that exercise simply burns calories, and deepen our understanding of the complex interactions of physical activity and metabolism.
Kindle edition, now available!
Great news - The Decision Tree is now available in a Kindle e-reader edition at Amazon.com! Here's the link: Decision Tree on Kindle
The Book Hits the Store
Whew, what a week. The Decision Tree debuted to some great acclaim and attention, and I think it's useful to update some of the highlights here
Whew, what a week. The Decision Tree debuted to some great acclaim and attention, and I think it's useful to update some of the highlights here.
Freakonomics blog @ NYTimes.com: A q/a with the Freaknomics blog about decision making, when screening makes sense, and the utility of genetic testing.
Big Money: I Wanna CT Scan Your Hand: An excerpt that discusses how the high price of CT scans adds to healthcare costs.
TheAtlantic.com: The Wonder Drug Myth: Another excerpt, this one about the infrequently discussed miss-rate of drugs.
BoingBoing: An astute read of the book by Bill Guerstelle.
Gizmodo on Sleep Gadgets: A piece I wrote for them about how gadgets like sleep trackers can help us monitor and improve our health.
Also, I'm grateful to power tweets from Tim Ferriss, Dan Pink, Steve Case, Deepak Chopra, and countless others. Hopeful for another big week!
Can High Blood Glucose Levels Cause Cancer?
Diets high in simple sugars and refined carbs cause metabolic disorders and Type II diabetes in millions of Americans. But to make matters worse, new evidence suggests that high sugar diets may be even more dangerous than we initially thought. Having too much excess sugar in the bloodstream is never a good thing, and can lead to medical complications such as kidney failure, cardiovascular disease, and eye problems. But could high blood sugar also cause cancer? A Swedish research team addressed this question by tracking over 500,000 patients for 10-25 yeas, and published their results in the December issue of PLoS Medicine.
Diets high in simple sugars and refined carbs cause metabolic disorders and Type II diabetes in millions of Americans. But to make matters worse, new evidence suggests that high sugar diets may be even more dangerous than we initially thought. Having too much excess sugar in the bloodstream is never a good thing, and can lead to medical complications such as kidney failure, cardiovascular disease, and eye problems. But could high blood sugar also cause cancer? A Swedish research team addressed this question by tracking over 500,000 patients for 10-25 yeas, and published their results in the December issue of PLoS Medicine.
Similar to the findings of a study conducted in Korea in 2005, the European research team discovered that having elevated blood glucose levels increased the risk of developing certain types cancer later in life, such as pancreatic tumors in women and liver tumors in men. Not only had more cases of cancer occurred when people had high blood sugar, but the chance of survival also plummeted, especially when the person had cervical, espohageal, or colorectal cancers.
The authors present two theories on why elevated blood glucose levels could cause cancer: 1.) high sugar diets may cause an overproduction of insulin or insulin-like growth factor 1 (IGF-1), both of which promote rapid growth of new cells, the catalyzing step to tumor formation. 2.) More glucose in the blood stream could simply be adding fuel to the fire, feeding rogue tumor cells that need lots of energy to run.
Because the studies lacked certain controls, we can't say for sure whether elevated blood glucose levels cause certain tumors to form. For example, the people with high blood glucose levels may have been sedentary, and so the lack of exercise may be what's actually increasing the chances of developing cancer. Regardless, this study gives yet another example of unhealthy lifestyles contributing to comorbidity, a topic discussed at length by Thomas in The Decision Tree book.
Is Self-Guided Research Dangerous to Your Health?
There are patients - and then there are active patients. And some of the people I talked to for my book I'd call veryactive patients. They have struck out on their own and made radical decisions about their healthcare. Teri Smieja is one of these heroes. When she learned that she had a genetic risk for breast and ovarian cancer, she embarked on a series of decisions - illustrated beautifully in this excerpt in Wired Magazine - that resulted in her getting two preemptive surgeries

There are patients - and then there are active patients. And some of the people I talked to for my book I'd call veryactive patients. They have struck out on their own and made radical decisions about their healthcare. Teri Smieja is one of these heroes. When she learned that she had a genetic risk for breast and ovarian cancer, she embarked on a series of decisions - illustrated beautifully in this excerpt in Wired Magazine - that resulted in her getting two preemptive surgeries.
Todd Small is another. A 40-something Seattle father who happens to have multiple sclerosis, Todd first came to my attention when I reported a story about Patientslikeme.com for the New York Times Magazine. At the time, Todd was actively engaged in his medication - he learned from his fellow PatientsLikeMe community members that his dosage for a drug called baclofen was probably too low, and adjusted it accordingly (working with his doctor, I hasten to add).
When I checked back in with Todd recently while reporting the book, I was surprised to hear that he was about to embark on an even more radical decision: he had heard about an experimental stem cell treatment for MS, and was about to give it a whirl. Todd, who admits he’s no whiz at science, couldn’t make out what the research was saying. So he turned to the PatientsLikeMe community. “If somebody could decode this into simple layman’s terms, it would be much appreciated,” he posted in an online forum.
Soon enough, his fellow members did decode the research - and the consensus seemed to indicate that the procedure, though somewhat risky, was a reasonable bet. It was nothing to sniff at: the treatment begins by extracting 400 milliliters—a little more than a can of soda—of bone marrow from the leg. For several weeks, those cells are used to grow more cells, after which the patient returns and about 50 million cells are injected into the spinal column. The cells seem to repair some of the damaged myelin in the central nervous system, lessening the symptoms of MS. About 60 patients had been treated with the procedure, and 55 had reported major improvements in their symptoms, including a former Canadian golf pro who was able to return to the game.
To Todd, the idea “was a no-brainer,” he told me later. “I just gotta go for it. If I don’t do this, I’ll be kicking myself. And in another year, I’ll have to quit my job at the shop. I have a family. I have two kids. I owe it to them to at least try this.”
Such self-guided research unnerves the medical establishment. That way, they warn, quickly leads to quack cures and dangerous treatments. That’s no doubt true in many arenas. But the power of PatientsLikeMe is that its members take their science seriously. They demand published research, not anecdotes. They’re quick to debunk phony cures and quackery. They consider themselves not just beneficiaries of research, but participants in an ongoing research project.
PatientsLikeMe co-founder Jamie Heywood calls this “personalized research.” On a smartly run, well-organized Web site, patients can play a huge role in informing each other; they can decentralize and distribute information that once was available only through a personal physician. This means that people can share not only their stories but also best practices and results. The crowd can create its own research, becoming what Jamie describes as “an insight engine.”
The same spirit propels CureTogether, a Web site that lets people with dozens of conditions, from allergies to vulvar vestibulitis, track their treatments and symptoms. Like PatientsLikeMe, CureTogether has an insatiable appetite for tracking patient data, and a faith in collaborative insight. “It’s driven by the patients, not by scientists.” Carmichael calls the insights that result from the nearly 7,000 members at CureTogether “collective wisdom.”
PatientsLikeMe and CureTogether can be seen as a direct challenge to physicians’ omniscience: The companies not only let members track their disease progression, they tacitly encourages them to try to turn those progression curves in a positive direction. This is what's unnerving to many doctors. But it's also what makes the self-guided approach so compelling. When it's done with data, when it's done as a feedback loop, it can actually result in good, more informed decisions.
Not all of these approaches are right for everyone. Constant self-tracking of the sort that PatientsLikeMe requires—updating one’s symptoms and dosages and progress—can be tedious, especially for somebody who already has a chronic illness. And not everyone is the “early adopter” type. But the truth is, you don’t have to be an early adopter to understand the virtues of mindfulness. At their best, Web sites like PatientsLikeMe and CureTogether offer a true middle path—one that has a grounding in science, yes, but also an understanding that we ordinary folk tend to look to each other, rather than textbooks or research papers, for advice on how to lead and improve our lives. The stories we share about our lives, especially stories about our health, can be incredibly powerful.
The key is to combine our affinity for stories and narrative with our capacity for rational decision making. It's in the combination where there's relevance, and where there's relevance, there's an occasion for action.
How To Make Better Decisions For Your Health
Every day, we make dozens of decisions without thinking about them: what to feed the kids, how fast to drive to work, whether to hit the snooze bar. We make most of these decisions without a second thought. We go with our gut.

Quick snip of my latest post on Huffington Post, which is generating a terrific response today.
Every day, we make dozens of decisions without thinking about them: what to feed the kids, how fast to drive to work, whether to hit the snooze bar. We make most of these decisions without a second thought. We go with our gut.
For other decisions, though, we have to pause, consider our options, and bring our best judgment to bear. This can be uneasy territory -- and it can get especially fraught with decisions about our health, when we often lack a strategy for weighing all the information on the table. We're not sure where to start.
But making smart decisions about our health doesn't have to provoke anxiety. It turns out we're well equipped to consider a range of options and make the right call. We just need to keep a few principles in mind.
T-Minus 1 Day: A Progress Report
In these days before the book comes out - tomorrow! - there have been some wonderful write-ups about the book. Just thought I should note them here. Kent Bottles wrote a piece titled "Check Lists and Decision Trees" that mulled whether structures like a decision tree can help people negotiate the huge information dumps that come with data-driven medicine. Besides the flattering proximity to Atul Gawande's book, Bottles was generous in grasping the fact that I'm not claiming a decision-tree paradigm depends solely on rational decision making (which is inevitably unrealistic) but that I'm trying to find a way to bring our rational capacity together with our emotional needs - and therein lies better healthcare.
In these days before the book comes out - tomorrow! - there have been some wonderful write-ups about the book. Just thought I should note them here. Kent Bottles wrote a piece titled "Check Lists and Decision Trees" that mulled whether structures like a decision tree can help people negotiate the huge information dumps that come with data-driven medicine. Besides the flattering proximity to Atul Gawande's book, Bottles was generous in grasping the fact that I'm not claiming a decision-tree paradigm depends solely on rational decision making (which is inevitably unrealistic) but that I'm trying to find a way to bring our rational capacity together with our emotional needs - and therein lies better healthcare.
Brian Ahier wrote a terrific post on O'Reilly Radar, largely about the book. Riffing off one of my set phrases - it's data, not drugs - Brian - who's not only a health IT expert and blogger but also a member of his city council - nailed the promise and riddle of turning to a data-intensive model for healthcare. As he puts it, "Putting the patient at the center of healthcare and creating a strategy to process all of health data available today is a great start towards meaningful healthcare reform." I was especially glad that Brian recognized the flexibility of my three principles for patient-centric health: Early is better than late; Let data do the work; and Openness is a powerful thing.
And Susannah Fox of the Pew Center lobbed a characteristically provocative take recently on e-patients.net. Her take: that the book could be retitled What to Expect When Your Expecting a Long Life. (Fine with me; those What to Expect books are huge!). In addition to the flattering notion that the Decision Tree compelled Susannah - a longtime health expert - to rethink her own health decisions, she astutely recognizes that I'm not just calling for self-tracking gadgets and gizmos - I'm really arguing that we should use whatever tools we have, including messaging from the FDA and other official bodies - to make health information clearer and more personalized.
It's very heartening to me that three people who constitute experts in the field all seem to think the book is in tune with their own knowledge - that the notes are right, and that the composition is in the right key. My hope, of course, is that the book will also find a larger, less-expert audience, but my hunch is that unless I convince the experts, the lay audience won't be there. If these three are any indication, I'm on the right track.
Lastly, I want to address some Twitter kibbitzing that these ideas are simplistic, naive, or somehow dangerous. I take some assurance that so far, this chatter comes from people who haven't read the book - because the book itself goes to great lengths to explore both the promise as well as the perils and challenges of engaging in patient-centric healthcare (challenging both for the patient and the system). There is ample evidence presented in the book; the bibliography alone runs to 15 pages. Of course, I'll answer this head-on when I have the chance. But broadly, I'll offer this:
There is hope in the book, yes; there is a simplicity to the idea, indeed - but naive or simplistic it is not.
The Quantified Pregnancy
An insightful post by Susannah Fox of the Pew Internet Project called "What's the Point of Health 2.0" was stuck in my mind all week. For the people already living their lives as "e-patients", the concepts we talk about here at The Decision Tree simply make sense. They'll say, "Of course I should track some aspect of my personal health". Or, "Why wouldn't I engage with other people on the internet who have a similar medical condition as me?" But what about the rest of the people out there? How can I best convince them of the power of the Health 2.0 movement? In her post, Susannah said that Esther Dyson helps her understand that even though the Health 2.0 crowd is relatively small right now, these e-patients provide a glimpse of how powerful and interactive health care can become in the future.
An insightful post by Susannah Fox of the Pew Internet Project called "What's the Point of Health 2.0" was stuck in my mind all week. For the people already living their lives as "e-patients", the concepts we talk about here at The Decision Tree simply make sense. They'll say, "Of course I should track some aspect of my personal health". Or, "Why wouldn't I engage with other people on the internet who have a similar medical condition as me?" But what about the rest of the people out there? How can I best convince them of the power of the Health 2.0 movement? In her post, Susannah said that Esther Dyson helps her understand that even though the Health 2.0 crowd is relatively small right now, these e-patients provide a glimpse of how powerful and interactive health care can become in the future.
For similar reasons, expecting moms give me hope for the future of Health 2.0. They constantly read up on the latest baby health information. They post comments on blogs, forums, and social networks, sharing insider tips and trends.
Last week, I attended the quasi-monthly San Francisco Quantified Self meetup. We had yet another spectacular night of presentations by people who are tracking some aspect of their life, whether it's health data, fitness trends, or a complex analysis of how they spend every minute of the day. The meetup was hosted by MedHelp, a company that's created a large medical social community. I was particularly struck by their presentation on their suite of personal health trackers, which included a 'Pregnancy Symptom Tracker'.
With MedHelp's online application, women can easily track the symptoms they're experiencing, such as morning sickness, fainting incidents, and mood swings. But in true Web 2.0 fashion, the true power of the application is realized when users share their data with others. By pooling the data of many users, MedHelp is defining, in near real-time, the norms of pregnancy. For example, their results show that morning sickness peaks around week 8, but falls off rather quickly later in the pregnancy. Fainting spells are far more common right before birth than at any other time. Alas, there's no relief from mood swings. They occur in 40% of women, and are fairly constant while pregnant.
I hope that in the future, data like this will arm people with the information to decide if a certain symptom is normal, or whether it's time to see a doctor. After all, making decisions based on data will not only help people save dollars at the doctor's office, but will also lead to better health.



More on Calculators: Harvard Does the Math
After my recent post on the Healthcare Blog about calculators (aka nomograms) for risk assessment and treatment guidance, I got an email from James Michaelson at the Laboratory for Quantitative Medicine (what a name!) at Harvard Medical School. He pointed me to some calculators they've cooked up - and they are simply outstanding, pushing far beyond anything I've seen out there otherwise. The lab's philosophy is centered around something it calls "binary biology", and the mission statement is fascinating:

After my recent post on the Healthcare Blog about calculators (aka nomograms) for risk assessment and treatment guidance, I got an email from James Michaelson at the Laboratory for Quantitative Medicine (what a name!) at Harvard Medical School. He pointed me to some calculators they've cooked up - and they are simply outstanding, pushing far beyond anything I've seen out there otherwise. The lab's philosophy is centered around something it calls "binary biology", and the mission statement is fascinating:
Each of us is but the aggregate consequence of the enormous number of fundamentally discrete events that occur among the many molecules, genes, and cells of which we are comprised. For more than a decade, our group has used this viewpoint to try to make sense of multicellular organization and its diseases.
I love the embrace of randomness, the almost existentialist detachment of it. And of course, it's exactly right: We have consciousness, but we are but biological machines. The fact that we think we're unique and supreme individuals with some sort of higher purpose is what so often leads us astray, especially when making healthcare decisions. It turns out that when given a prognosis - say a 15% chance of a drug working - we tend to assume that we're going to be in the 15% for whom it works rather than the much-more-likely 85% for whom it doesn't. Psychologists call this "illusory superiority," or the "Lake Wobegon effect," after Garrison Keilor's riff on a place where "...all the children are above average."
Some people may take this as depressing or even nihilistic sentiment, but I actually find it somewhat empowering: It basically says, OK - we're all just some cell functions and protein expressions and chemical interactions. So how well can we understand those functions and interactions, how can we quantify them, in order to best predict how they will combine to our specific circumstance? Now that's a calculator I want my doctor to have.
Like the nomograms at Memorial Sloan Kettering, the LQM has some cancer calculators. Under the rubric of CancerMath.net, there are therapy, outcomes and survival calculators for breast cancer, melanoma, and renal cell carcinoma. And over at PreventiveMath.net there's a splendid calculator that determines best practices for people based on their age, gender, smoking status, height and weight. This calculator largely draws on my favorite assessment source, the US Preventive Service Task Force recommendations. But the outcomes are delivered in a clear and easy-to-understand form: by "days of life added."
So if I, a 41 year old, 5-foot-11-inch, non-smoking male who weighs 155 pounds, were to begin taking a baby aspirin a day, I'd gain 286 extra days of life (on average), and if I were to get assessed for hypertension I'd gain 139 days. It's pretty powerful stuff. (my only complaint is a title like "PreventiveMath.net" is going to scare some people off). Here's a screenshot of the clean, clear interface:
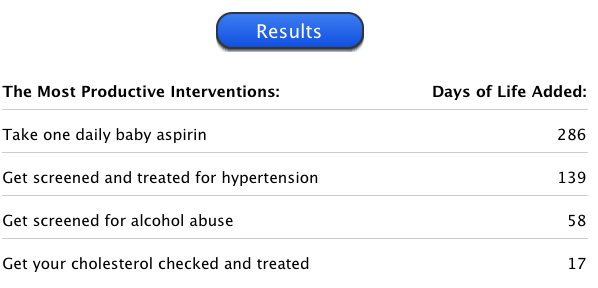
And each of these listed items is a hotlink to more information. Check out the Lab's full set of tools and statements at LifeMath.net. I'm sorry I didn't know about Dr. Michaelson's group earlier, so that I could include these terrific tools in my book. Still, I'm glad to get the word out here.