Life, Liberty, and the Pursuit of Affordable Health Care
In my opinion, our inalienable rights should be restated as the title of this post suggests. But despite my wishful thinking, health care costs continue to rise. By 2030, the boomer generation will place 57.8 million people in the 66-84 age group, further burdening current government funding for Medicare. The outlook is bleak, and the system needs fixing. One idea for lowering health care costs is to move health services out of the clinic, and into the home. New web-based services and personal diagnostic equipment now enable patients to receive medical care from the comfort of their living room. Is it realistic this model will reduce costs and stick? I'll cover the web-based services in this post, and follow up with another post on home diagnostic equipment. Web-based doctor's appointments are now available in several states. For example, at $10 per month, and $50 per consultation, SwiftMD offers an online health care plan in New York and New Jersey. Within 30 minutes of scheduling an appointment, subscribers have either a phone conversation or an online video chat with an available physician. If prescriptions are required, the physician sends the request electronically to the pharmacy of the subscriber's choice. A step further in service, Hello Health adds conveniences such as the ability to text, instant message, or tweet your doctor, and also offers clinic appointments or house calls for more serious conditions. Both SwiftMD and Hello Health do not cover major medical expenses, so if the subscriber has to go to the emergency room or be admitted to the hospital, the cost is theirs. Also, neither accepts insurance, but compared to ever increasing health insurance premiums and the number of uninsured patients, an affordable "pay for what you need" model may just work.

In my opinion, our inalienable rights should be restated as the title of this post suggests. But despite my wishful thinking, health care costs continue to rise. By 2030, the boomer generation will place 57.8 million people in the 66-84 age group, further burdening current government funding for Medicare. The outlook is bleak, and the system needs fixing. One idea for lowering health care costs is to move health services out of the clinic, and into the home. New web-based services and personal diagnostic equipment now enable patients to receive medical care from the comfort of their living room. Is it realistic this model will reduce costs and stick? I'll cover the web-based services in this post, and follow up with another post on home diagnostic equipment. Web-based doctor's appointments are now available in several states. For example, at $10 per month, and $50 per consultation, SwiftMD offers an online health care plan in New York and New Jersey. Within 30 minutes of scheduling an appointment, subscribers have either a phone conversation or an online video chat with an available physician. If prescriptions are required, the physician sends the request electronically to the pharmacy of the subscriber's choice. A step further in service, Hello Health adds conveniences such as the ability to text, instant message, or tweet your doctor, and also offers clinic appointments or house calls for more serious conditions. Both SwiftMD and Hello Health do not cover major medical expenses, so if the subscriber has to go to the emergency room or be admitted to the hospital, the cost is theirs. Also, neither accepts insurance, but compared to ever increasing health insurance premiums and the number of uninsured patients, an affordable "pay for what you need" model may just work.
A recent article highlighted the services of Hello Health, and discussed the ways electronic media is reshaping health care. More important than describing cool, new ways to communicate with your doctor, and boutique concierge services offered by modern clinics, the article does a fine job pointing out the importance of social networking in the future of health care. Physicians use websites such as Sermo and UpToDate to stay abreast of advances in health care and treatment, as well as to network with other doctors in the field. Patients, on the other hand, have traditionally been stuck with tools such as WebMD, NIH's MedlinePlus, and the Mayo Clinic site, all of which just give background information on diseases, and pave the way for dangerous self-diagnosis.
Such patient websites provide little help to the proactive patient who is curious if others with a certain condition are experiencing similar symptoms or medication side effects. Enter PatientsLikeMe, a website that focuses on user-generated data (via self monitoring and reporting) and lets others know what to expect on the road ahead. PatientsLikeMe provides a useful social networking community if you are already diagnosed with a condition, but what if you are a 40-something male with a BMI of 28, blood pressure at 135/85, and recently diagnosed with metabolic syndrome? Is there anyone out there with similar stats that can offer information about what regiments have kept them healthy? In other words, let's not wait until we are diagnosed with heart failure to seek out advice from our peers -- we need social networking tools when we are still just "at-risk" for the disease.
While electronic access to your physician is much cheaper than going to an office visit, to truly drive health care costs down, we need to increase the personal responsibility of the public -- we need to heighten our medical knowledge, track our own body metrics, and pool our data. Social networking sites provide the necessary framework to disseminate such information and personal experiences across large populations. Armed with the proper information, patients will be able to make their own decisions about their health. Now that's a true health care revolution -- so go tweet your way to better health. I'll discuss home diagnostic testing soon...
Science as a Search Function
The ideal combination of the internet and science is to put data (lots of data) into a easily/readily searched database. The hypothesis becomes a search: Want to know what people are prone to which disease? Want to know what genetic backgrounds compell certain behaviors? Run a search. That's the ideal - and though this idea has been hashed about for a few years, we're a long way from there now. There is no such database out there, an ongoing research project that combines enough data and enough flexibility in interogation and enough variety in populations that it might adequately reflect a broad enough pool of data to be meaningfully searched.
The ideal combination of the internet and science is to put data (lots of data) into a easily/readily searched database. The hypothesis becomes a search: Want to know what people are prone to which disease? Want to know what genetic backgrounds compell certain behaviors? Run a search. That's the ideal - and though this idea has been hashed about for a few years, we're a long way from there now. There is no such database out there, an ongoing research project that combines enough data and enough flexibility in interogation and enough variety in populations that it might adequately reflect a broad enough pool of data to be meaningfully searched.
Until, perhaps, today. Or tomorrow.
On Thursday, 23andMe will announce a project with the Michael J. Fox Foundation and the Parkinsons Institute and Clinical Center that will enroll up to 10,000 people with Parkinson's Disease, get them genotyped using 23andMe platform, and then issue them a survey to fill in the phenotypic information - the physical "end result" correlation to our genotypic information - to make for a rich and fruitful database. This database will then be ripe for interrogation, and with members' permission, it will be searched and probed for possible correlations and implications. 10,000 is a big number for Parkinson's Disease, and such a large population will afford, it's hoped, a rich enough database to afford meaningful implications. (Linda Avey, 23andMe cofounder, describes the effort here).
The idea is to create a genetic database around one disease - Parkinson's - that is rich and robust and big enough to answer lots of questions that get into minutae: If this isn't a "genetic disease" (ie, typically brought on purely by genetic cause), then what are the fractions of effects caused by our genomes? It's a complicated question, but if we're really going to get to an understanding and application of predictive medicine, then we need to understand all the possible inputs that have ramifactions into a multitude of outputs.
This is, in effect, the thing that's been talked about for about 5 years now: Googling our Genomes. And it's not surprising that behind this landmark endeavor is Google, or at least its co-founder, Sergey Brin. Brin, who has said he has a genetic risk for Parkinson's, has funded the study and promised to give 10,000 people their genomic data for just $25 each (the 23andMe service is regularly about $400). So that's at least a $4 million commitment, at least at the going rate of genotyping - and that's not counting the backend research that will take place. Brin will also be a participant in the study.
I don't doubt that many folks will be skeptical of this endeavor (Valleywag and Steve Murphy, start the race to be the first to squat on this with some snide remark, starting...now!) And sure, I acknowledge that 23andMe is good at publicity. But I think there's a fundamental shift in science here that should not go unnoted.
This is an endeavor to create an apparatus for answers; answers not just to the questions we have today, but the questions science will have or 10 years from now. This is, indeed, science by search. And I'm thrilled that somebody's actually trying to make it happen. And here's what's especially cool: 23andMe co-founders Ann Wojcicki and Linda Avey know this is what they're doing. They talk about this as a "research platform," and they have a host of diseases that they want to hit next: Autism, Alzheimer's, and so on. Expect more this year.
Again, this isn't a research study - this is a new way to study research. Make the costs of research recruitment (finding populations to study, recruiting individuals, taking samples, and repeating every time you have a new question to ask) a backend function, and prioritize the questions, not the apparatus. It's how to do science in the petabyte age.
I'll add some more tomorrow, including some remarks from Wojcicki and Avey.
A New Model for Predictive Medicine Practitioners: Physical Therapists
Suffering an orthopedic injury can be devastating. It can preclude us from athletic competition or force us to take time off work, not to mention the added strain it puts on completing normal daily tasks while partially immobilized or in pain. Regardless if surgery is required, a physical therapy rehabilitation program is usually prescribed to aid recovery. Say hello to countless hours of sweat, pain, and foul language (primarily in the form inner monologue, often directed toward the therapist that you are certain is trying to tear your limbs from your body, but occasionally a choice expletive might just slip out in frustration or exhaustion). Well, not necessarily, says Caitlin Kelly, who recently blogged about what she felt was the unsuspecting upside of physical therapy-- the healing power of the friendships formed during the sessions. Day after day, through all the pain and suffering, she got to know and relate to other patients, and maybe even more importantly, developed an open-communication relationship with her therapists. Ultimately, the injury healed, and the unforeseen personal bonds persisted long after the pain subsided.
Suffering an orthopedic injury can be devastating. It can preclude us from athletic competition or force us to take time off work, not to mention the added strain it puts on completing normal daily tasks while partially immobilized or in pain. Regardless if surgery is required, a physical therapy rehabilitation program is usually prescribed to aid recovery. Say hello to countless hours of sweat, pain, and foul language (primarily in the form inner monologue, often directed toward the therapist that you are certain is trying to tear your limbs from your body, but occasionally a choice expletive might just slip out in frustration or exhaustion). Well, not necessarily, says Caitlin Kelly, who recently blogged about what she felt was the unsuspecting upside of physical therapy-- the healing power of the friendships formed during the sessions. Day after day, through all the pain and suffering, she got to know and relate to other patients, and maybe even more importantly, developed an open-communication relationship with her therapists. Ultimately, the injury healed, and the unforeseen personal bonds persisted long after the pain subsided.
Aside from their good interpersonal skills, physical therapists seem to have a knack for treating the person, not just the condition. Every patient has different questions, concerns, strengths, and weaknesses, making it nearly impossible to have a canned treatment program that will work in every situation. I've had the fortunate experience of working with some really great physical therapists over the years, and not only do I believe they were instrumental in helping me recover from injury, I believe they prevented future injuries from occurring by preemptively addressing other issues. For example, at one point I was chronically pulling the same hamstring. While not career ending, or severe in the grand scheme of sports injuries, it still prevented me from competing. No matter how much hamstring stretching/strengthening I did, I couldn't shake the problem. It wasn't until my physical therapist told me that I need to address the tightness in my hip flexors that I was able to prevent the injury from occurring. At first, this made no sense to me. Why would stretching a muscle on the front of my leg help prevent an injury on the back of my leg? They explained that tightness in the hip flexor could be negatively impacting my stride, and leading to the hamstring pull.
Physical therapists are an excellent model of the new-wave health practitioner, since custom treatments that address the patient's past, present, and (potential) future health, together with an open dialogue between the health provider and patient, are the heart and soul of personalized medicine. We've been bugging physicians to do these things for a while, and it's refreshing to see a health practitioner that's already got it under control.
Recently I had a great conversation with some friends and colleagues who brought up an interesting point: the experiences I had with my physical therapists, they've had with other health practitioners -- massage and acupuncture therapists, yoga instructors, dietitians, and personal trainers. Predictive medicine will require our own team of health practitioners, only a few of which are physicians. There are many people who can aid our quest to stay healthy, and implementing our own Decision Trees will require tapping into all of these resources.
Cheeseburgers on the Mind
Making a choice that leads to better health is not always easy. Otherwise, we would have many more ex-smokers and far fewer holiday pounds to shed. We would have no need for nicotine gum and patches, or Weight Watcher's meetings. So if it's that difficult, why bother? For years, physicians have told the American public that reducing your calorie intake, eating a diet low in salt/sugar/saturated fat, and exercising 3-5 days per week will reduce your risk for heart disease and diabetes. Now, new information has shown that the benefits of a healthy lifestyle are even more far reaching than initially thought -- diet and exercise can affect our minds. About 5-8% of people over the age of 65, and nearly 50% of people in their 80's, show signs of dementia. As the baby-boomer generation increases the population of the 55-64 age group in the U.S. from 29 to 40 million by 2014 , and their life expectancy continues to rise, the number of people affected by dementia is poised to increase as well. Recent studies have shown that regular exercise may prove to be a potent mediator of dementia and Alzheimer's Disease. In one study, those who exercised 3 or more days per week had a 32% risk reduction in developing dementia compared to those who exercised less. Exercise has also been linked in similar studies to moderate cognitive improvements in adults who are at risk for Alzheimer's Disease, as well as a lower occurrence of vascular dementia.
Making a choice that leads to better health is not always easy. Otherwise, we would have many more ex-smokers and far fewer holiday pounds to shed. We would have no need for nicotine gum and patches, or Weight Watcher's meetings. So if it's that difficult, why bother? For years, physicians have told the American public that reducing your calorie intake, eating a diet low in salt/sugar/saturated fat, and exercising 3-5 days per week will reduce your risk for heart disease and diabetes. Now, new information has shown that the benefits of a healthy lifestyle are even more far reaching than initially thought -- diet and exercise can affect our minds. About 5-8% of people over the age of 65, and nearly 50% of people in their 80's, show signs of dementia. As the baby-boomer generation increases the population of the 55-64 age group in the U.S. from 29 to 40 million by 2014 , and their life expectancy continues to rise, the number of people affected by dementia is poised to increase as well. Recent studies have shown that regular exercise may prove to be a potent mediator of dementia and Alzheimer's Disease. In one study, those who exercised 3 or more days per week had a 32% risk reduction in developing dementia compared to those who exercised less. Exercise has also been linked in similar studies to moderate cognitive improvements in adults who are at risk for Alzheimer's Disease, as well as a lower occurrence of vascular dementia.
Recent pre-clinical results have shown that diet is also tied to brain health. A 2002 study revealed that rats fed a diet high in saturated fat and refined sugar for 2 years exhibited changes in both gene expression in the brain, as well as performance on a memory task (finding its way through a water maze). This fast-food type diet decreased the levels of brain-derived neurotrophic factor (BDNF), which is a versatile molecule that mediates brain cell formation, function, and survival. Both BDNF gene expression (mRNA) and BDNF protein production in the hippocampus, an area crucial for short-term memory, were significantly reduced in the animals fed the high-fat and refined sugar diet, compared to those on a low-fat, complex carbohydrate diet. Although the experiment lasted for 2 years, and the greatest effects were seen at the end of the experiment, changes in gene expression were seen in as little as 6 months after the rats began downing cheeseburgers. Even more striking, the rats had a significant deficit in the water maze memory task after only 3 months on the high fat/sugar diet, which shows that the "McDiet" led to a change in behavior in the mice.
Nevertheless, the research presented here had limitations. The studies that looked at the effects of exercise on dementia were conducted in relatively small, non-diverse human populations and were not completely controlled against other "good health" factors that tend to occur when people exercise. For example, exercisers are much more likely to do other healthy things, such as eating right, quitting smoking, getting quality sleep, or maintaining target weight. The fast-food diet study was well controlled to show that decreased BDNF was not related to hypertension, atherosclerosis, obesity, and changes in activity level -- but the results must be taken at face value since it was conducted in rodents, not humans.
So what does all of this mean? The idea of eating right and getting more exercise is nothing new. We've known for years that changing our health behaviors can stave off heart disease, and potentially let us live longer. The studies mentioned here really highlight the positive-feedback nature of our actions -- behavior changes (diet and exercise) cause physiological and molecular changes in the body, which in turn alter another behavior (memory). This relationship tells us that our behavior choices no longer only determine life or death, but they also can impact our quality of life. It's true that the results don't make a direct link between diet/exercise and brain health, but rather, a loose correlation between the two that requires further study. But in my mind, it doesn't really matter what keeps the brain healthy -- my point isn't that diet and exercise are the end-all cure for disease, but rather, that they are an extremely important part of an overall healthy lifestyle that will allow us to make the most of our golden years.
Lost in Translation: The Disconnect Between Scientists and the Public
The NewScientist recently blogged about C.P. Snow's idea of "two cultures": those trained in the sciences and those trained in the humanities. In this 1959 lecture, Snow proposed that a communications chasm between these groups hindered the effort to solve the world's problems with new technology. He concluded that the two groups essentially spoke different languages that made it impossible to identify common goals. Snow's lecture captured the proverbial differences in "left vs. right brains", and showed us that scientists need to be better at communication while non-scientists need to be more conversant in basic technical and scientific concepts.
The NewScientist recently blogged about C.P. Snow's idea of "two cultures": those trained in the sciences and those trained in the humanities. In this 1959 lecture, Snow proposed that a communications chasm between these groups hindered the effort to solve the world's problems with new technology. He concluded that the two groups essentially spoke different languages that made it impossible to identify common goals. Snow's lecture captured the proverbial differences in "left vs. right brains", and showed us that scientists need to be better at communication while non-scientists need to be more conversant in basic technical and scientific concepts.
Fifty years later, Snow's original idea that these "two cultures" are not communicating still holds true. In my work at various medical technology companies, I've often heard engineers and scientists complain that the business folks don't grasp the technical ideas. Similarly, those on the business side get frustrated with the engineer's or scientist's obsession with small inconsequential details, rather than stepping back and looking at the big picture.
How does this issue relate to The Decision Tree? In previous posts, we’ve talked about the necessary behavioral changes that individuals must make in order to put the concepts of The Decision Tree into practice -- and I realize that's asking for a lot. From collecting and analyzing your body metrics to increasing your medical/scientific knowledge, implementing your decision tree will no doubt be demanding. At the same time, both physicians and scientists should translate their work into insights that resonate with the general public. In a previous post, we talked about MedEncentive's interest in improving doctor-patient communication. Similarly, a better scientist-patient relationship will enable better health decision-making. This way the scientific professionals and general public could find a middle ground to address the rift described by Snow, thus bridging "the two cultures". More after the jump.So how do we improve communication between scientists and non-scientists? We (society) rely on scientists to push the boundaries of medical/scientific innovation and understanding. As a result, society puts a certain amount of trust in these people to ethically conduct research and get results. In return for the trust (and funds, via tax dollars sent to agencies such as NIH), I believe the public 1.) deserves to see the results via access to scientific publications, and 2.) is owed a reasonable explanation of what the research is all about.
The idea of sharing results publicly through "open" research is hardly a new thought. Currently, open research broadly refers to the fact that published data should be accessible to everyone, not just those who pay the fees to subscribe to the right journals. To solve this problem, journal article repositories are emerging, such as PubMed Central, to which authors must submit new articles (2008 onward) arising from NIH funded grants within 1 year of publication. A step even further is an organization such as The Public Library of Science (PLoS), which has been an open access publisher since its inception, and makes published research in medicine and biology available to all readers.
But what good is access when the research itself is beyond understanding? Scientists are terrible communicators, and as a scientist myself, I often struggle with papers or talks loaded with details and jargon. In science, understanding the details of one's own research, and being able to effectively express your idea and findings to others, seem to be two completely independent skill sets. I've seen scientific experts flounder when giving a presentation to people outside their area of expertise. I don't think anyone in the room doubted the speakers knew what they were talking about, but something was getting lost in translation, so to speak. The funny thing was, in many instances, the audience was filled with other scientists, only a different specialty than the speaker. So not only do scientists have trouble communicating with non-scientists, they also have trouble communicating with each other.
In scientific publications, the abstract of the article is supposed to be a summary of the study, but often the complexity of the paper simply carries through to this paragraph-long synopsis of the work. A better approach might be something such as PLoS Medicine editors' summary. These are readable summary statements written by the editorial staff that specifically address questions such as "Why was this study done" or "What do these findings Mean". These high-level summaries give readers a brief, but complete, overview of the study. Scientists should be able to write these types of summaries themselves. This skill would benefit a scientist's own career, since their work would reach a much larger audience.
Here's how these changes would benefit individuals: If someone has a risk for Condition X, they could find out if preclinical research studies identified new potential therapeutic targets. If your grandfather and uncle both died of Condition Y, you could be on the lookout for new biomarkers that might bear promise, and perhaps genetic links emerged between Conditions X and Y that warrant watching out for. People would be empowered with this information, simply by knowing that they understand the work on the leading edge of treatment of their relevant conditions, or how these findings could directly impact their life.
Reforming health care will demand the interaction of all people – left brains and right brains. We need everyone to grasp concepts in fields such as genetics, statistics, health nomenclature, and physiology -- at least enough to make proper decisions about their health. Therefore, transforming society into an evidence-based mindset will inevitably require the interpretation of newly published data. I believe the scientific community can aid the transition of the next-generation patient, but they just need a little nudge to start thinking about the ways they express themselves.
The Risks (and Rewards) of Risk Assessment Tools
The New York Times had a story on Friday criticizing the National Cancer Institute for its new decision tool on colon and rectal cancers. The problem, the reporter says, is that the tool - an interactive questionaire that creates a risk estimate for developing colon cancer - only works for white people. African-Americans or Hispanics who try the tool get a message that says: “At this time the risk calculations and results provided by this tool are only accurate for non-Hispanic white men and women ages 50 to 85.” It's an odd story for a couple reasons. First, the reporter seems to have created the controversy on her own - she quotes only one critic of the tool, and that critic is described as reacting negatively "after being referred to the site by a reporter." The same reporter, I assume, who's writing the story. Hmm.

The New York Times had a story on Friday criticizing the National Cancer Institute for its new decision tool on colon and rectal cancers. The problem, the reporter says, is that the tool - an interactive questionaire that creates a risk estimate for developing colon cancer - only works for white people. African-Americans or Hispanics who try the tool get a message that says: “At this time the risk calculations and results provided by this tool are only accurate for non-Hispanic white men and women ages 50 to 85.” It's an odd story for a couple reasons. First, the reporter seems to have created the controversy on her own - she quotes only one critic of the tool, and that critic is described as reacting negatively "after being referred to the site by a reporter." The same reporter, I assume, who's writing the story. Hmm.
But the real problem with the critique is that it barely acknowledges the reason that the tool only works for whites: It's because the data on risk for colon cancer that's built into the site is based on research that only studied whites. In other words, the NCI used the existing epidemiology, the data that exists, which is based on a Caucasian population study. More research is being done on risks in other populations, but it's not substantial enough to merit a valid decision tool.
I'm all for calling on the NCI to extend the tool and fund the science that will relate to more people. But this is the way of all research - you take certain populations, which correlate in various ways to larger populations, and try to ascertain risk. Rare is the study that's so well funded and so well managed that it can handle the full spectrum of people in the US. So the science evolves slowly, piece by piece, and over time the broader population is covered. Yes, there is such a thing as disparities in health research - certain populations are regrettably understudied. But there's no indication in the Times story that that's the case with colon cancer.
So the Times story has the effect of criticizing the NCI for creating a tool because it's incomplete, entirely missing the forest for the trees: The great thing here is that such a tool exists in the first place. This is the sort of thing we should be encouraging the NCI and other health entities to do - show us the science, and show us how it's relevant, *as it emerges and as soon as it emerges*. These sorts of risk assessment tools are incredibly powerful ways for individuals to think about their health. They help us understand the great body of science in immediately personal terms, giving us perspective on how our decisions - in this case, how much exercise we get or how many vegetables we eat - affect our risk for developing cancer. This should be applauded and encouraged, not criticized for failing to emerge in an all-at-once exhaustive form.
Indeed, the one critique that I have about the NCI's tool - which you can see here - is that it doesn't make plain how your risk stands up against other people's, nor does it make plain what sort of changes could reduce your risk. When I played around with a worst-case scenario for me - only some exercise and not many vegetables - it gave me a lifetime risk of about 6%. But without the context of a general population, I have no idea if that's high or low. And when I fiddle with the numbers and say I take aspirin and eat lots of vegetables and get lots of exercise, my lifetime risk drops to 1.6%. Much better, but I had to guess at what variables to change - meaning I have to guess at what changes to make to my life to improve my odds. If the NCI automated these functions and let me know where I stood and what I might consider changing, the tool would be a lot more potent.
Automatic Data Tracking with Personal Health Monitors
I started thinking about the usefulness of personal health monitors last year. Heart disease runs rampant through my family, and several of my maternal uncles have had heart attacks, one of them at the age of 35. With my 30th birthday rapidly approaching, I started to think about my own mortality -- my blood pressure and cholesterol were both already well above average. Given my family's history of heart disease, I decided to go talk to my general physician. We decided the best course of action was to treat the problem with diet and exercise modifications. Although I have been physically active my entire life, I realized that I no longer had the metabolism of a teenager, and had to start thinking about what I was eating and how I was exercising before there was a serious impact on my health.And so, I began running again for the first time in a very long while. I knew that as I ran more and more, I would start to just feel "better", but that notion just wouldn't satisfy the science geek inside me, and I needed to put numbers to my improvements. So I started tracking my heart rate (via a standard chest-strap heart rate monitor ). I figured, at the very least, tracking my heart rate (HR) during my run would allow me to understand how it correlated to my exertion level. It would also be interesting to see how my HR changed as I got back into shape. I bought the basic version -- the one that shows your current heart rate, but doesn't store any of the data or calculate statistics like max/min/average HR. I was surprised how consistent my HR was during exercise, and soon began to use this information to gauge the intensity of my runs. For example, some days I would be feeling fine and I would be running at my normal pace, but my HR was running about 3-4% higher than usual. While I'm not sure if that is abnormal, it happens very infrequently, and I used it as a signal that I should slow down and take it easy. While my current understanding of my HR during exercise is far from the interpretation of body metrics talked about here at The Decision Tree, I believe my analysis has me headed in the right direction.
I started thinking about the usefulness of personal health monitors last year. Heart disease runs rampant through my family, and several of my maternal uncles have had heart attacks, one of them at the age of 35. With my 30th birthday rapidly approaching, I started to think about my own mortality -- my blood pressure and cholesterol were both already well above average. Given my family's history of heart disease, I decided to go talk to my general physician. We decided the best course of action was to treat the problem with diet and exercise modifications. Although I have been physically active my entire life, I realized that I no longer had the metabolism of a teenager, and had to start thinking about what I was eating and how I was exercising before there was a serious impact on my health.And so, I began running again for the first time in a very long while. I knew that as I ran more and more, I would start to just feel "better", but that notion just wouldn't satisfy the science geek inside me, and I needed to put numbers to my improvements. So I started tracking my heart rate (via a standard chest-strap heart rate monitor ). I figured, at the very least, tracking my heart rate (HR) during my run would allow me to understand how it correlated to my exertion level. It would also be interesting to see how my HR changed as I got back into shape. I bought the basic version -- the one that shows your current heart rate, but doesn't store any of the data or calculate statistics like max/min/average HR. I was surprised how consistent my HR was during exercise, and soon began to use this information to gauge the intensity of my runs. For example, some days I would be feeling fine and I would be running at my normal pace, but my HR was running about 3-4% higher than usual. While I'm not sure if that is abnormal, it happens very infrequently, and I used it as a signal that I should slow down and take it easy. While my current understanding of my HR during exercise is far from the interpretation of body metrics talked about here at The Decision Tree, I believe my analysis has me headed in the right direction.

After a year of using the HR monitor, I feel I am ready for an upgrade. I want the data collection to be automated. There is a new class of personal health monitors that is intended to not only be used during exercise, but rather, can be worn throughout the day. These devices passively collect data, and require no input from the user. So as you carry on your daily life -- walking to meetings, running to catch the bus or train, moving your friend's sofa up 3 flights of stairs -- these monitors are automatically calculating metrics such as the total calories burned, steps taken, and miles traveled. Combined with online calorie trackers, these devices create a one-stop diet and exercise analysis system. I just wanted to briefly outline 3 devices that are either on the market, or will be this year. I have chosen these products for their flexibility (you can wear them with any clothing, and can even collect information while you sleep).
GoWearFit is an armband which has sensors to measure skin temperature and moisture, as well as body acceleration. The company's software uses the data collected from all of the sensors to determine metrics such as calories burned, physical activity duration, steps taken, sleep duration, and sleep efficiency. Periodically, the user must take off the armband and plug it into their computer to upload their data to the GoWearFit website. There is an online subscription required to view your data on your personal activity manager site. So the consumer must pay an upfront cost for the armband (~$150+), and then pay the monthly cost for viewing their data (~$7-13, depending on the service contract).

In pre-release sale now, FitBitis a small device that clips on an waist band, shirt, or a wrist strap (provided by the company). It tracks calories burned, steps taken, miles covered, and sleep quality. When the user walks within 20-50ft of the provided basestation, the data is wirelessly transferred, so there is no need to take the device off and connect it to a computer. The basestation then transfers the data to a personal online database. Unlike the GoWearFit system, with FitBit the user pays $99 for the device and that's it -- no monthly subscription fee to view the data. Screen-shots of the online health manager are available on the company's website, and include some nice features, such as a "see what your friends are up to" social networking tool, which could provide some motivation to go to the gym after those long days, when you are struggling to find the reason you started exercising in the first place.

SportBrain has similar features to the FitBit, such as tracking calories, miles, steps, and even has an online personal community where the user can track the activity of family and friends. One nice addition is that it also integrates with certain heart rate monitors. It appears the device is not wireless, so it must be taken off and connected to your computer to upload the data.
Changing Our Energy Habits, By the Numbers
A brief tangent: I'm at the TED conference this week, and today I put on my editor hat and moderated a panel on how to change our global energy priorities, by moving away from oil/gas towards renewables. On the panel were two luminaries - Richard Sears, a VP at Shell and visiting scientist at MIT, and Dan Reicher, head of energy initiatives at Google.org (Dan was a member of the Obama transition team and on the shortlist, reportedly, to be Obama's secretary of energy). The lunch went well - among others, Bill Gates was in the audience - and it seemed a lively discussion about what can actually be done, right now, to incentivize both the oil industry as well as consumers to start the shift to other energies.

A brief tangent: I'm at the TED conference this week, and today I put on my editor hat and moderated a panel on how to change our global energy priorities, by moving away from oil/gas towards renewables. On the panel were two luminaries - Richard Sears, a VP at Shell and visiting scientist at MIT, and Dan Reicher, head of energy initiatives at Google.org (Dan was a member of the Obama transition team and on the shortlist, reportedly, to be Obama's secretary of energy). The lunch went well - among others, Bill Gates was in the audience - and it seemed a lively discussion about what can actually be done, right now, to incentivize both the oil industry as well as consumers to start the shift to other energies.
The consumer angle is especially intriguing, given the focus of The Decision Tree, since one of the items most often mentioned as a driver towards better consumer behavior - in terms of moving towards conservation and making smarter more efficient energy choices - is metrics. Reicher mentioned that the Obama stimulus package, as originally written, has something like $4 billion earmarked to go towards buying (or help buying) some 40 million smart meters for households. That's enough to change one in three households towards smarter energy usage. Smart meters are basically feedback devices that let consumers know how much energy they're using and at what times, allowing them to adjust their consumption habits to consume less (and spend less).
This is, readers will recognize, the same sort of thing that's emerging as significant for changing our health behaviors - giving people a way to see and measure, quantitatively, what they're doing - and then to calibrate adjustments. Even better: Provide for openness, and let people compare and collaborate on improving their behaviors.
A couple cool examples in the energy world are Fuelly, a website with a social networking component that let's you track how much you drive your car, what sort of mileage you're getting, and so on. This is the province of so-called hypermilers, but also folks who just want to drive less and spend less on gas - which was pretty much all of us over the summer. Another cool tool here is WattzOn (pronounced "watson"), a site developed by Saul Griffith that lets you track your overall energy consumption, from airplane travel to food production to consumer goods like clothing. OK, this borders on obsessive, and isn't entirely practical - but it does give a remarkable picture of our overall energy footprint - not just our carbon footprint - and might provide ways we could cut back (Griffith, for instance, rations the amount of airplane trips he'll go on each year).
So the parallels here are quite neat - in both circumstances (health and energy), new tools are emerging that suddenly turn our invisible lives into stark, bold numbers, numbers that we can give us insight into exactly where we stand, as well as direction for where we might want to go. In both cases, it's not going to be easy to actually stick to our principles and change how we do things. It's no easier to stop driving than it is to stop eating (or in the case of In 'n' Out burger, doing both at once). But gaining perspective on the relationship between our actions and our greater context - be it our health or our planet's health - is a necessary first step.
Improving Your Medical Literacy
The ideas behind The Decision Tree, in a sense, focus on ways to create the next-generation patient. This new kind of patient will have to understand the context of their own medical self through a combination of genetics, personal metrics/data, and statistics. Needless to say, understanding one's own medical self will also require an increased medical literacy, where patients understand both their conditions, as well as where they fall within the spectrum of their disease.
The ideas behind The Decision Tree, in a sense, focus on ways to create the next-generation patient. This new kind of patient will have to understand the context of their own medical self through a combination of genetics, personal metrics/data, and statistics. Needless to say, understanding one's own medical self will also require an increased medical literacy, where patients understand both their conditions, as well as where they fall within the spectrum of their disease.
Creating the next-generation patient will inevitably require new tools. Website services, such as PatientsLikeMe, have been a step in the right direction towards increasing patient knowledge by empowering people with general knowledge of their conditions, as well as and providing information of what others in their shoes are experiencing. However, focusing on the patient may only address half of the problem.
MedEncentive, a start-up company founded in 2003, approaches the issue of medical literacy by addressing both players in the problem, the physician and the patient. MedEncentive's product focuses on developing, or even better, redefining, the doctor-patient relationship. A statistic listed on their website states that on an average office visit, the physician will interrupt the patient within seconds of entering the room, while the patient only comprehends a fraction of the information given to them by their doctors. Drawing from my own mixed experiences dealing with physicians – including a recent diagnosis botched 3 times in a week – I could see how this could be true. If a patient had an increased understanding of their conditions, perhaps this interaction would not be so one-sided.
The company's core product is an incentive program for doctors and patients that centers around the exchange of medical information. Doctors who participate in the medical literacy program can earn about 20% more (~$15) per office visit by assigning their patients a "to-do" list. The company mentions some of what this list might include, such as questionnaires which determine how much a patient understands about both their current health status and the conditions they've been diagnosed with, as well as how they would rate their doctor's performance. The patients earn rewards, such as copay reimbursements or health savings account credits, for completing their reading assignments and the questionnaires.
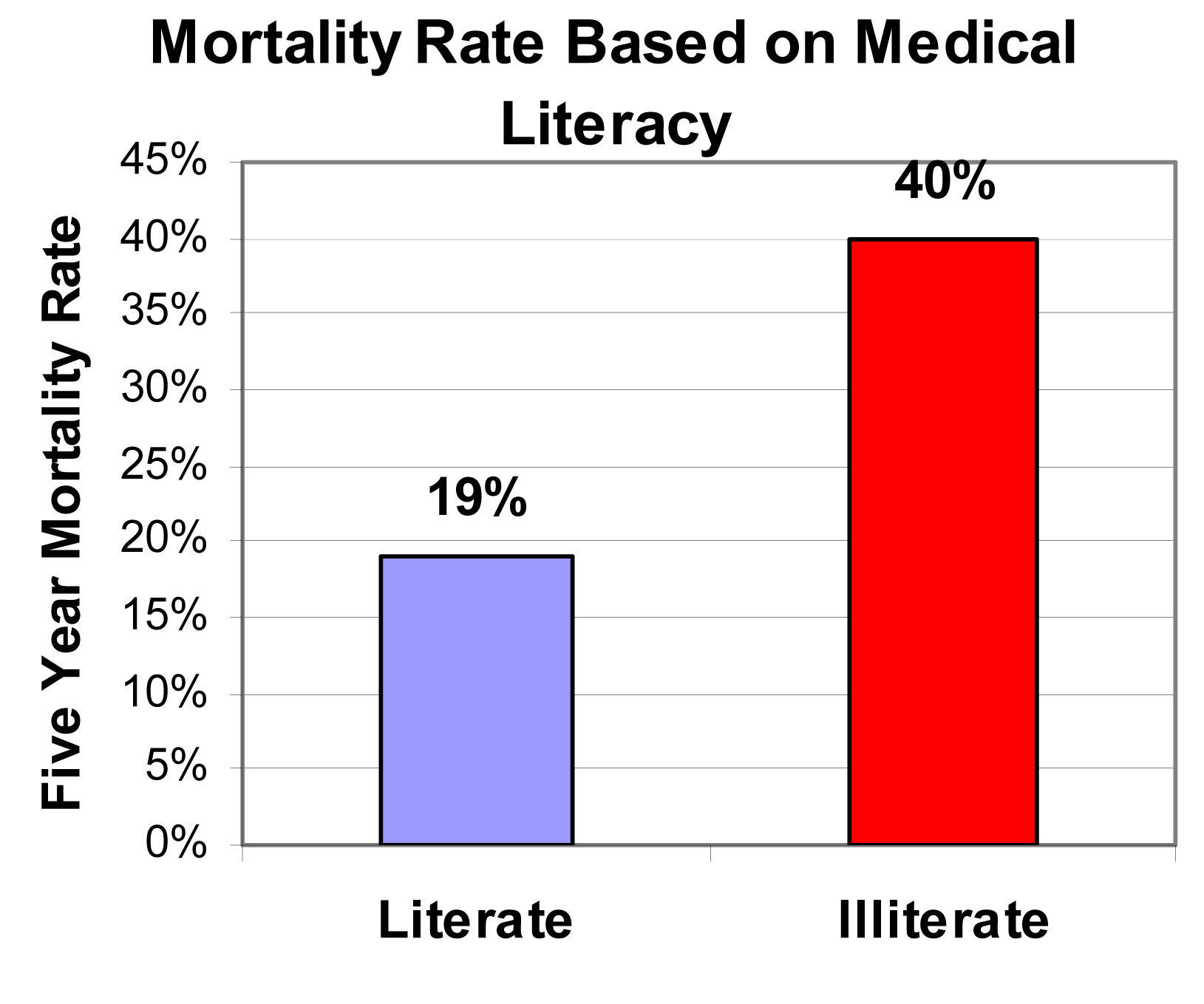
According to the company, a medically literate patient will communicate more efficiently with their physician, while medically illiterate patients will consume more health care resources. But do people really care about this? Sure, it would be nice to reduce health care costs and make doctors and patients best friends, but is it really a big deal if a patient doesn't understand the ins-and-outs of their conditions? If you are not sold on the benefit of developing the doctor-patient relationship, consider the following figure. It was taken from a study conducted by physicians at Northwestern University and Emory University on the 5-year mortality rate of an elderly population. Medical illiteracy can become dangerous when it leads to an increased risk of death. So based on the outcome of this study, MedEncentive's thesis makes sense: when patients know more about their medical conditions, they have better health.
I acknowledge that there is a confounder to this study -- it was conducted in an elderly population. As we all know, the cognitive abilities of the elderly vary drastically across the population. For example, your 90-year old grandfather may be self-sufficient, living on his own, and sharp as a tack, while my 90-year old grandmother requires assisted living. So one question I asked myself when looking at this study was: are the people who are in the medically illiterate group also the ones who are in assisted living? In other words, is the increased risk of death due to the fact that the patient doesn't understand medical jargon, or is it due to an overall decline in their mental capabilities? Luckily, the clinical team already addressed this question. They found that both an increased medical literacy and a higher cognitive ability both independently indicated a longer, healthier life. So those that understand their medical conditions will live longer, but so will those who can still do the New York Times crossword puzzle themselves.
My take: The benefits of medical literacy, as outlined here, are: 1.) knowledge can improve the doctor-patient relationship, and 2.) knowledge can improve health. The Decision Tree is not about a single factor influencing a healthy life, rather it discusses a collective set of behavioral changes that lead to new way to think about and treat disease. I think the results discussed here show that medical literacy is an important piece of the next-generation patient puzzle. In the future, we will be asking a lot from patients, as more of the responsibility for staying healthy will be shifted to them. So I like the approach of MedEncentive to get the doctor involved as well. In the end, what we end up with is the next-generation patient, as well as a new breed of physician -- one who is willing to break the current mold.
Introducing a New Contributor: Brian Mossop
Though predictive medicine and preventive health are common sense to some people, sometimes I have the feeling that I'm shouting into a hurricane about how the right tools & the right information can change healthcare. So I'm always thrilled - truly thrilled - when somebody tells me: "I read what you wrote - and I've been thinking the same thing." A couple years ago I had this experience when I got an email from a fellow with some astute questions about my approach to writing about science. Except this wasn't a journalist - this was from a scientist. And that both flattered and scared me. Flattered, in that a bonafide PhD took my stuff seriously. Scared, in that a bonafide PhD was reading my blog - and taking it seriously.
Though predictive medicine and preventive health are common sense to some people, sometimes I have the feeling that I'm shouting into a hurricane about how the right tools & the right information can change healthcare. So I'm always thrilled - truly thrilled - when somebody tells me: "I read what you wrote - and I've been thinking the same thing." A couple years ago I had this experience when I got an email from a fellow with some astute questions about my approach to writing about science. Except this wasn't a journalist - this was from a scientist. And that both flattered and scared me. Flattered, in that a bonafide PhD took my stuff seriously. Scared, in that a bonafide PhD was reading my blog - and taking it seriously.
This fellow's name was Brian Mossop, and he proved an especially intriguing guy. I've spent 20 years figuring out how to keep abreast on the zeitgeist, but this guy - in his mid-20s - seemed to already be surfing the wave. He got the power, the promise, and the pitfalls of healthcare technology. And he understood that the real power of medicine wasn't when it was deployed on a one-to-one basis, but when it could be catylized to hundreds or thousands. In other words, giving people access to information could be more important than the creation of that information (research) in the first place.
And so we kept talking. And sure enough, when I came around to the whole Decision Tree idea, Brian Mossop was one of the first on board. Not only did he get what I was talking about, he was already starting to research the same stuff - predicitive medicine, personal metrics, genomic data, health information in the hands of the individual - all on his own.
Well, this made no sense to me. He didn't even have a blog, & here he was thinking the same stuff. So now he has a blog. This blog. I'm proud and happy and once again flattered to announce that Brian Mossop will be joining me here at TheDecisionTree.com, blogging about the frontiers of health care. And in the process, he'll be helping lay out the themes and particulars that I'll be exploring in the book.
Here are his bonafides: Brian received a BS in Electrical Engineering from Lafayette College, and a PhD in Biomedical Engineering from Duke University in 2006, where he worked on electric field-mediated gene and drug delivery, primarily for cancer treatment. He did postdoc work at UCSF, then a few a Bay Area companies, and now he focuses on basic neuroscience and neurodegenerative disease (using electrophysiology and imaging). He won't be blogging about his day-job here - he's here strictly as a science-savvy informed observer of where data and openness and prediction are taking our healthcare system.
In his own words: "The concepts behind the Decision Tree will help create a more proactive healthcare system, where consumers and patients take initiative in the prevention and treatment of disease. I have worked in multidisciplinary teams since moving into the biomedical field, and I have learned that progress is best made when you look at problems from different points of view. I hope to continue this philosophy here at the Decision Tree, and leverage my scientific training to address some of the issues facing the rise of predictive medicine in society."
It's a real thrill to have such a partner in making this blog all it can be. Please make Brian welcome - but hold him to the same standards you would me. In other words, feedback is welcome.